Neurologische Untersuchung der oberen Gliedmaßen
Begutachtet von Dr Philippa Vincent, MRCGPZuletzt aktualisiert von Dr Toni Hazell, FRCGPZuletzt aktualisiert 20. Mai 2026
Erfüllt die Anforderungen des Patienten Richtlinien des Patienten
- HerunterladenHerunterladen
- Teilen
- Language
- Diskussion
- Audio-Version
- Zu bevorzugten Quellen bei Google hinzufügen
Medizinische Fachkräfte
Fachartikel sind für die Nutzung durch Gesundheitsfachkräfte konzipiert. Sie werden von britischen Ärzten verfasst und basieren auf Forschungsergebnissen, britischen und europäischen Richtlinien. Möglicherweise finden Sie einen unserer Gesundheitsartikel nützlicher.
Es gibt mehr als eine Möglichkeit, eine neurologische Untersuchung durchzuführen, und ein Kliniker sollte seine eigene Technik entwickeln. Eine schlechte Technik wird keine Anzeichen hervorrufen oder falsche Ergebnisse liefern.
Siehe auch das separate Neurologische Anamnese und Untersuchung article which covers the basic principles of examination and technique.
Examination of the upper limbs may be performed more easily with the patient sitting in a chair or standing.
Inspection of the upper limbs1
Note if there appears to be any damage to the hands.
On inspection, note the following:
The resting posture. Note whether there is unusual rotation or clawing of the hand and whether anything about the patient is asymmetrical.
Look for muscle wasting or hypertrophy. Note whether it is focal or diffuse.
Achten Sie auf unwillkürliche Bewegungen wie Tremor, Tics, myoklonische Zuckungen, Chorea oder Athetose.
Look for muscle fasciculation (sign of lower motor neurone disease process). These are subcutaneous twitches over a muscle belly at rest. Tapping the belly may stimulate fasciculation.
Upper limb examination of the sensory system
Examination of each of the sensory modalities:1
Leichte Berührung
Verwenden Sie die sanfte Berührung eines Fingers, ein Stück Watte oder ein Stück Papiertaschentuch.
Es ist wichtig, zu berühren und nicht zu streicheln, da eine Bewegungsempfindung, wie Reiben und Kratzen, über Schmerzbahnen geleitet wird.
Bitten Sie den Patienten, die Augen zu schließen und Ihnen zu sagen, wann er Ihre Berührung spürt.
Vergleichen Sie jedes Glied in der gleichen Position.
Halten Sie das Timing jeder Berührung unregelmäßig, um eine Vorwegnahme durch den Patienten zu vermeiden.
A logical progression is required. You may want to start testing over the shoulder and to move along the lateral aspect of the arm and up the medial side, as this moves progressively from C4 to T3 dermatomes.
Notieren Sie alle Bereiche von Hypoästhesie oder Dysästhesie.
Scharfer Berührungstest (Nadelstich)
Testen Sie mit einem speziellen Einwegstift. Eine Einweghypodermische Nadel ist zu scharf.
Verwenden Sie den Brustbeinbereich, um eine Basislinie für die Schärfe festzulegen, bevor Sie beginnen.
Follow the same progression as with light touch with the patient's eyes closed, comparing both upper limbs.
Bitten Sie den Patienten, Hypoästhesie (fühlt sich stumpfer an) oder Hyperästhesie (fühlt sich schärfer an) zu melden.
Temperatur
Dies wird oft übersehen, kann aber wichtig sein.
An easy and practical approach is to touch the patient with a tuning fork as the metal feels cold.
Vergleichen Sie die Qualität der Temperaturempfindung an Armen, Gesicht, Rumpf, Händen, Beinen und Füßen.
Behälter mit warmem und kühlem Wasser können für eine genauere Beurteilung verwendet werden. Bitten Sie den Patienten, mit geschlossenen Augen zwischen warm und kühl auf verschiedenen Hautbereichen zu unterscheiden.
Gelenkstellungssinn (Propriozeption)
Test at the distal interphalangeal joint of the index finger.
Hold the middle phalanx with one thumb and finger and hold the medial and lateral sides of the distal phalanx with the other. Move the distal phalanx up and down, showing the patient the movement first.
Bitten Sie den Patienten, die Augen zu schließen und die distale Phalanx zufällig nach oben und unten zu bewegen. Bitten Sie den Patienten, Ihnen jedes Mal die Bewegungsrichtung zu nennen.
Test on both hands.
If there is an abnormality, move backwards to the proximal interphalangeal joint and so on until joint position sense is normal.
Vibrationssinn
Verwenden Sie eine 128 Hz Stimmgabel und stellen Sie sicher, dass die Stimmgabel vibriert.
Platzieren Sie es zunächst auf dem Brustbein, damit der Patient das Gefühl spüren kann.
Then place it on one of the distal interphalangeal joints of one of the fingers.
If no vibration is sensed, move backwards to the metacarpophalangeal joint, the wrist, etc.
Den Patienten zu bitten, Ihnen mitzuteilen, wann die Stimmgabel aufhört zu vibrieren, kann hilfreich sein, wenn Zweifel bestehen, ob ihr Vibrationsempfinden intakt ist.
Two-point discrimination
There are specific two-point discriminators available. If you don't have one, use a paper clip that you can open out.
Ask the patient to close their eyes.
Take the patient's index finger in one of your hands.
Using the discriminator or paper clip, touch the pulp of the finger with either one or two of the testing tips.
The patient must tell you whether they can feel one or two stimuli.
Find the minimum distance at which they can discriminate the two tips. Normal is at 3-5 mm.
Compare both index fingers and repeat for both thumbs.
Upper limb examination of the motor system2
Tonus
This is the resistance felt when a joint is moved passively through its normal range of movement:
Ask the patient to let their shoulders and arms 'go floppy'.
Flex and extend their shoulder passively and feel for abnormality of tone.
Repeat for the elbow and wrist.
Hypertonia is found in upper motor neurone lesions; hypotonia is found in lower motor neurone lesions and cerebellar disorders.
Cogwheel rigidity may be found in Parkinson-Krankheit.
Kraft3
Eine robuste Bewertung der Leistung ist erforderlich.
The Medical Research Council (MRC) has a recommended grading system for power (see table). It has been shown to have good reliability although doubts have been expressed over the wide range of grade 4.
Die manuelle Muskeltestung wird unterschiedlich bewertet mit 4 - Gut: voller Bewegungsumfang gegen die Schwerkraft mit mäßigem Widerstand, und 5 - Normal: voller Bewegungsumfang gegen die Schwerkraft mit maximalem Widerstand.
Ask the patient to contract the muscle group being tested and then you as the examiner try to overpower that group.
Testen Sie Folgendes:
Abduction, adduction, flexion and extension of the shoulder.
Flexion and extension of the elbow.
Flexion and extension of the wrist.
Supination and pronation of the forearm.
Extension of the fingers at the metacarpophalangeal and interphalangeal joints.
Flexion, extension, adduction and abduction of the fingers and thumbs.
MRC-Skala für Muskelkraft
0 | Keine Muskelkontraktion ist sichtbar. |
1 | Muskelkontraktion ist sichtbar, aber es gibt keine Bewegung des Gelenks. |
2 | Aktive Gelenkbewegung ist möglich, wenn die Schwerkraft eliminiert wird. |
3 | Bewegung kann die Schwerkraft überwinden, aber nicht den Widerstand des Prüfers. |
4 | Die Muskelgruppe kann die Schwerkraft überwinden und sich gegen einen gewissen Widerstand des Prüfers bewegen. |
5 | Volle und normale Leistung gegen Widerstand. |
Tiefe Sehnenreflexe
Stellen Sie sicher, dass der Patient bequem und entspannt ist und dass Sie den zu testenden Muskel sehen können.
Verwenden Sie einen Reflexhammer, um die Sehne des Muskels zu schlagen und auf eine Muskelkontraktion zu achten.
Vergleichen Sie beide Seiten.
Reflexe können hyperaktiv (+++), normal (++), träge (+) oder abwesend (-) sein. ± wird verwendet, wenn der Reflex nur bei Verstärkung vorhanden ist (siehe unten).
In the upper limbs:
Test the biceps jerk (C5, C6): with their arm relaxed, hold the patient's elbow between your thumb and remaining fingers, your thumb being anterior and directly over the biceps tendon. Ideally the elbow should be held at 90°. Elicit the reflex by tapping on your thumb.
Test the triceps jerk (C6, C7): with their arm relaxed, hold the patient's arm across their lower chest/upper abdomen with one of your hands. Elicit the reflex by tapping over the triceps tendon just above and behind their elbow.
Test the supinator jerk (C5, C6): ask the patient to relax their arm across their abdomen. Elicit the reflex by tapping over the supinator tendon just above the wrist.
Test the finger jerk: with their hand relaxed, place the tips of your index and middle fingers across the palmar surface of the patient's proximal phalanges. Tap your fingers lightly with the tendon hammer. There should be slight flexion of the patient's fingers. If there is hyperreflexia, this flexion is exaggerated.
Test the Hoffmann's reflex: rest the distal interphalangeal joint of the patient's middle finger on the side of your right index finger. Use the tip of your right thumb to flick down on the patient's middle fingertip. Watch for any movement of the patient's thumb as their fingertip springs back up. Normally there is no movement; in hyperreflexia, thumb flexion can be seen.
If a reflex is difficult to elicit, try 'reinforcement' (the Jendrassik manoeuvre). Ask the patient to clench their teeth or squeeze their knees together while you try to elicit the reflexes again.
Interpretation
Obere Motoneuronläsionen führen normalerweise zu Hyperreflexie.
Untere Motoneuronläsionen führen normalerweise zu einer verminderten oder fehlenden Reaktion.
Isolated loss of a reflex can point to a radiculopathy affecting that segment - eg, loss of biceps jerk if there is a C5-C6 disc prolapse.
Untersuchung der Koordination
The cerebellum helps in the co-ordination of voluntary, automatic and reflex movement. Tests of cerebellar function, however, are only valid if power and tone are normal, and that failure to perform them may also be related to power and tone abnormalities in the upper limb rather than a cerebellar problem. These include:
The finger-nose test:
The patient should keep their eyes open.
Hold one of your fingertips up in front of, and a short distance (about 30-40 cm) from, the patient.
Ask the patient to touch the tip of their nose and then to touch your fingertip alternately and repeatedly. You can continuously change your fingertip position to make the test more difficult.
You can then test for sensory ataxia by asking the patient to close their eyes and to touch the tip of their nose using their outstretched finger.
Repeat these tests on the other side.
Look for intention tremor and past-pointing as the patient touches the examiner's fingertip, which can indicate disease of the cerebellar hemispheres.
Rapid alternating movement:
The patient needs to have one palm facing upwards.
They need to touch this palm with the palmar and then dorsal sides of the fingertips of the other hand as quickly as possible. Note that they must lift the second hand between each movement and touch the same point on the other palm without rolling the hand.
Test both sides. It is normal for the dominant hand to be a little faster at this test.
Look for dysdiadochokinesis. This is inco-ordination or slow movement when trying to perform this test.
Neurologische Untersuchung
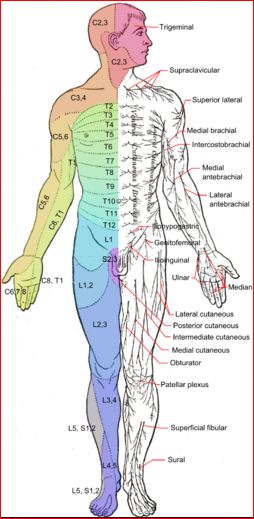
© Häggström, Mikael (2014). "Medical gallery of Mikael Häggström 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.008. ISSN 2002-4436. Public Domain
A note about sensation in the hand
The hand may require more intensive testing. It may be useful to return to it after testing the rest of the arm.
Test sensation on both the palmar and the dorsal aspects.
Be aware of the distribution of the median, ulnar and radial nerves:
The radial nerve supplies sensation to the skin on most of the dorsum of the hand.
The ulnar nerve supplies sensation to the palmar aspect of the little finger and the palmar aspect of the medial half of the ring finger. It also supplies the distal half of the dorsal aspect of these fingers.
The median nerve supplies sensation to the palmar aspect of the thumb, index and middle fingers and the lateral half of the ring finger. It also supplies the distal half of the dorsal aspect of these fingers.
Interpretation der Ergebnisse
The site of any lesion can be determined by looking at the pattern of any dysfunction found. The dermatomal (segmental) and peripheral nerve innervation is labelled in the diagram above.
All of the sensory modalities can be affected in peripheral neuropathies and nerve injuries, cervical radiculopathy and spinal injuries.
Wenn ein einzelner Nerv oder eine sensorische Wurzel betroffen ist, können alle sensorischen Modalitäten reduziert werden.
If there is a spinal cord lesion, there may not be equal diminution across all of the sensory modalities: light touch, vibration and joint position sense may remain intact while sharp touch and temperature are lost. This is because the lateral spinothalamic pathways may be damaged while the dorsal columns remain intact. Cervical Syringomyelie is an example where this may happen.
Problems with joint position sense or vibration usually occur distally first.
Das Vibrationsempfinden kann bei peripherer Neuropathie oder Myelopathie, die die Hinterstränge betrifft, vor dem Gelenkpositionssinn verloren gehen.
Parietal lobe lesions can also cause impairment of two-point discrimination.
The distal parts of the limbs tend to be affected in polyneuropathy, the legs usually being involved before the arms. A 'glove and stocking' effect is produced.
Exklusive Updates für medizinisches Fachpersonal
Bleiben Sie informiert mit den neuesten klinischen Updates, professionellen Einblicken und evidenzbasierten Leitlinien. Der Patient Pro-Newsletter stellt wesentliche Inhalte für Gesundheitsfachkräfte zusammen – direkt in Ihren Posteingang geliefert.
Durch das Abonnieren akzeptieren Sie unsere Datenschutzrichtlinie. Sie können sich jederzeit abmelden. Wir verkaufen Ihre Daten niemals.
Weiterführende Literatur und Referenzen
- Neurologische Untersuchung; Oxford medizinische Untersuchung (OME)
- Shahrokhi M, Asuncion RMD; Neurologic Exam
- Naqvi U, Sherman Al; Muscle Strength Grading
Über den AutorVollständige Biografie anzeigen

Dr Toni Hazell, FRCGP
MBBS, BSc, FRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell hat ihren Abschluss an der St. Mary’s Hospital Medical School gemacht und ihr VTS am Northwick Park Hospital absolviert.
Über den RezensentenVollständige Biografie anzeigen

Dr Philippa Vincent, MRCGP
Allgemeinmediziner, Medizinischer Autor
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent ist ein NHS-Arzt, der in Nordlondon arbeitet.
Artikelverlauf
Die Informationen auf dieser Seite wurden von qualifizierten Klinikern verfasst und begutachtet.
Artikel auch verfügbar in Englisch, Deutsch, Spanisch, Französisch, Italienisch, Portugiesisch, Hindi, Hebräisch, Arabisch, und Schwedisch.
Nächste Überprüfung fällig: 20. Nov 2030
20. Mai 2026 | Neueste Version

Fragen, teilen, verbinden.
Durchsuchen Sie Diskussionen, stellen Sie Fragen und teilen Sie Erfahrungen zu Hunderten von Gesundheitsthemen.

Fühlen Sie sich unwohl?
Bewerten Sie Ihre Symptome online kostenlos
Mehr in Geschichte und Untersuchung
- Rückenschmerzen bei Kindern
- Kardiovaskuläre Anamnese und Untersuchung
- Brustschmerzen
- Todesbescheinigung
- Dehydration bei Kindern
- Hepatomegalie
- Hiatushernie
- Schluckauf
- Pädiatrische Untersuchung
- Peripheres Ödem
- Pigmentierte purpurische Dermatitis
- Rektale Blutung bei Erwachsenen
- Sekundäre Kopfschmerzen
- Stridor
- Tenesmus
- Thyreoglossuszysten
- Tinnitus
- Tourette-Syndrom und andere Tic-Störungen
- Schwindel
- Xanthelasma