Ventrikuläre Tachykardien
Begutachtet von Dr Hayley Willacy, FRCGP Zuletzt aktualisiert von Dr Colin Tidy, MRCGPZuletzt aktualisiert 16. Okt 2024
Erfüllt die Anforderungen des Patienten Richtlinien des Patienten
- HerunterladenHerunterladen
- Teilen
- Language
- Diskussion
- Audio-Version
- Zu bevorzugten Quellen bei Google hinzufügen
Medizinische Fachkräfte
Fachartikel sind für die Nutzung durch Gesundheitsfachkräfte konzipiert. Sie werden von britischen Ärzten verfasst und basieren auf Forschungsergebnissen sowie britischen und europäischen Richtlinien. Sie finden möglicherweise die Unregelmäßige Herzrhythmen Artikel nützlicher oder einer unserer anderen Gesundheitsartikel.
What is ventricular tachycardias?
Ventricular tachycardia (VT) is a breiter Komplex-Tachykardie originating from a ventricular ectopic focus. It is defined as three or more ventricular extrasystoles in succession at a rate of more than 120 beats per minute (bpm). Accelerated idioventricular rhythm refers to ventricular rhythms with rates of 60-100 bpm:1
The rate is usually greater than 120 bpm with broad QRS complexes.
VT may be monomorphic (typically regular rhythm originating from a single focus with identical or similar QRS complexes) or polymorphic (may be irregular rhythm, with beat to beat variation in QRS complexes).
Monomorphic VT is the most common form of sustained VT.
Non-sustained VT is defined as a run of tachycardia of less than 30 seconds' duration; a longer duration is described as sustained VT.
Sustained VT is associated with:
Late phase of myocardial infarction (frequently with left ventricular aneurysm).
Cardiomyopathy (including hypertrophic and alcoholic).
Right ventricular dysplasia.
Myocarditis.
Drugs - eg, class 1 anti-arrhythmics (flecainide, and disopyramide).
Types of ventricular tachycardias
Fascicular tachycardia
Uncommon and not usually associated with underlying structural heart disease.
It originates from the left bundle branch.
It produces QRS complexes of relatively short duration (0.11-0.14 seconds) and so is commonly misdiagnosed as a supraventricular tachycardia (SVT).
The QRS complexes have a right bundle branch block pattern.
Right ventricular outflow tract tachycardia
Originates from the right ventricular outflow tract.
The ECG typically shows right axis deviation, with a left bundle branch block pattern.
The tachycardia may be provoked by catecholamine release, sudden changes in heart rate, and exercise.
It usually responds to drugs such as alpha-blockers or calcium antagonists.
Torsades de pointes tachycardia
Siehe das separate Torsades de pointes Artikel.
Polymorphic ventricular tachycardia
Has the same ECG characteristics as torsades de pointes but in sinus rhythm the QT interval is normal.
The ECG trace is also similar to that of atrial fibrillation (AF) with pre-excitation.
It is much less common than torsades de pointes.
If sustained, it often leads to cardiogenic shock.
It can occur in acute myocardial infarction and may deteriorate into ventricular fibrillation (VF).
How common is ventricular tachycardias? (Epidemiology)
VT is a fairly frequently observed dysrhythmia but actual incidence is difficult to quantify because of the overlap with VF. Shockable rhythms (pulseless VT and VF) are seen in about half of witnessed cardiac arrests in public locations where a defibrillator has been available.2 Coronary disease is the usual cause, which is common throughout most of the developed world.
VT incidence rates peak in the middle decades of life, following structural heart disease.
Risikofaktoren
VT is often a symptom of coronary heart disease or structural heart disease.
VT can be triggered by electrolyte deficiencies - eg, hypokalaemia, hypocalcaemia, hypomagnesaemia.
Use of sympathomimetic agents (eg, caffeine or cocaine) may stimulate VT in vulnerable hearts.
Präsentation
Most patients present with symptoms of either coronary heart disease or haemodynamic compromise resulting from poor perfusion.
Symptoms may include chest pain, palpitations, dyspnoea, dizziness, syncope and other symptoms of heart failure.
Signs reflect the degree of haemodynamic instability, including respiratory distress, basal fine lung crepitations, raised JVP, hypotension, anxiety, agitation, lethargy, and coma.
Differentialdiagnose
Other tachyarrhythmias, including narrow complex tachycardias, but more specifically other causes of breiter Komplex-Tachykardie:
ECG criteria that support VT over SVT include atrioventricular (AV) dissociation, fusion beats at the initiation of the arrhythmia, QRS duration over 140 ms, and RS pattern in V1. Patients with underlying structural or coronary heart disease are more likely to have VT than SVT.
ECG criteria that support SVT over VT include a right bundle branch block pattern, varying bundle branch block, an R or qR pattern in V1, or an ectopic P wave preceding the dysrhythmia.
Herzinsuffizienz from other causes.
Untersuchungen
EKG:3
Complexes of atypical morphology are often difficult to interpret. Such tachycardias could be paroxysmal supraventricular tachycardia (PSVT) with aberrant conduction. If the patient is unstable, or differentiation between VT and SVT is uncertain, treat rhythm as VT. Some therapies for PSVT (eg, verapamil) can be lethal when employed in VT.
No absolute ECG criteria exist for establishing the presence of VT. However, several factors suggest VT, including the following:
Rate greater than 100 bpm (usually 150-200).
Wide QRS complexes (>120 ms).
Presence of AV dissociation.
Fusion beats.
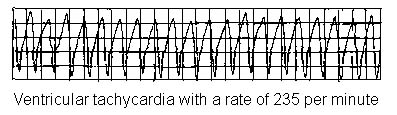
VENTRICULAR TACHYCARDIA
Retrograde ventriculoatrial conduction may occur, which can generate an ECG complex similar to PSVT with aberrant conduction.
Electrolytes, including serum calcium, magnesium, and phosphate levels. Ionised calcium levels are preferred over total serum calcium. Hypokalaemia, hypomagnesaemia, and hypocalcaemia may predispose patients either to conventional VT or torsades de pointes.
Levels of therapeutic drugs - eg, digoxin.
Evaluate for myocardial ischaemia: serum troponin I levels, or other cardiac markers.
CXR: if there is a possibility of congestive heart failure or other cardiopulmonary pathology as contributing factors.
Assoziierte Erkrankungen
Arrhythmia may occur with or without either myocardial ischaemia or infarction.
Accelerated idioventricular rhythm (sometimes termed slow ventricular tachycardia):
Presents with a rate of 60-100 bpm.
Typically occurs with underlying heart disease (coronary or structural).
It is transient, and only rarely is associated with haemodynamic compromise or collapse.
Treatment is usually not required unless there is haemodynamic impairment.
Ventricular tachycardias treatment
Address the ABCs of resuscitation and provide basic life support and advanced life support as necessary, urgent transfer to hospital, venous access, oxygen and ECG rhythm strip monitoring. See advanced life support algorithm.4
Pulseless VT
Is treated as for VF in line with the advanced life support algorithm.4
Unstable VT (reduced cardiac output)
Sehen adult tachycardia (with pulse) algorithm.4
VF or pulseless VT is treated by unsynchronised defibrillation; whereas other VTs can be treated with synchronised cardioversion.
Most patients respond to low levels of energy (eg, starting at 50 J biphasic or 100 J monophasic).
Synchronised defibrillation in unstable VT may cause R-on-T deterioration to VF.
Defibrillation is followed by airway management if required, supplemental oxygen, vascular access, and anti-arrhythmic therapy.
Advanced cardiac life support: amiodarone is often used for haemodynamically unstable VT. Replenishment of magnesium and/or other electrolytes may be a valuable adjunct to anti-arrhythmic therapies.
Stable VT
Stable VT patients do not experience symptoms of haemodynamic decompensation.
Unlike other dysrhythmias, VT tends to deteriorate into unstable states and more malignant dysrhythmias.
Therefore, stable VT should be treated with lidocaine or timely cardioversion if lidocaine is ineffective.
The evidence on percutaneous (non-thoracoscopic) epicardial catheter radiofrequency ablation for VT is limited but has shown that the procedure is effective in carefully selected patients and raises no major safety issues.5
Refractory VT
After the initial dose of amiodarone 300 mg IV, it may be followed by an infusion of 900 mg over 24 hours.4
Implantierbare Kardioverter-Defibrillatoren (ICDs)
National Institute for Health and Care Excellence (NICE) guidance recommends that ICDs should be considered for patients in the following categories:6
People with previous serious ventricular arrhythmia - that is, people who, without a treatable cause:
Have survived a cardiac arrest caused by either ventricular tachycardia (VT) or ventricular fibrillation; oder
Have spontaneous sustained VT causing syncope or significant haemodynamic compromise; oder
Have sustained VT without syncope or cardiac arrest, and also have an associated reduction in left ventricular ejection fraction (LVEF) of 35% or less but their symptoms are no worse than class III of the New York Heart Association (NYHA) functional classification of heart failure.
People who:
Have a familial cardiac condition with a high risk of sudden death, such as long QT syndrome, hypertrophic cardiomyopathy, Brugada syndrome or arrhythmogenic right ventricular dysplasia; oder
Have undergone surgical repair of congenital heart disease.
ICDs, cardiac resynchronisation therapy (CRT) with defibrillator (CRT‑D) or CRT with pacing (CRT‑P) may be considered as choices for people with heart failure who have left ventricular dysfunction with an LVEF of 35% or less.
Complications of ventricular tachycardias
Congestive cardiac failure and cardiogenic shock.
VT may deteriorate into VF.
Prognose
If treated rapidly, VT generally has a favourable short-term outcome.
Long-term prognosis depends upon the underlying cardiac disease.
Exklusive Updates für medizinisches Fachpersonal
Bleiben Sie informiert mit den neuesten klinischen Updates, professionellen Einblicken und evidenzbasierten Leitlinien. Der Patient Pro-Newsletter stellt wesentliche Inhalte für Gesundheitsfachkräfte zusammen – direkt in Ihren Posteingang geliefert.
Durch das Abonnieren akzeptieren Sie unsere Datenschutzrichtlinie. Sie können sich jederzeit abmelden. Wir verkaufen Ihre Daten niemals.
Weiterführende Literatur und Referenzen
- Whitaker J, Wright MJ, Tedrow U; Diagnosis and management of ventricular tachycardia. Clin Med (Lond). 2023 Sep;23(5):442-448. doi: 10.7861/clinmed.2023-23.5.Cardio3. Epub 2023 Sep 29.
- Cronin EM, Bogun FM, Maury P, et al; 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. J Arrhythm. 2019 May 10;35(3):323-484. doi: 10.1002/joa3.12185. eCollection 2019 Jun.
- Lopez EM, Malhotra R; Ventricular Tachycardia in Structural Heart Disease. J Innov Card Rhythm Manag. 2019 Aug 15;10(8):3762-3773. doi: 10.19102/icrm.2019.100801. eCollection 2019 Aug.
- Edhouse J, Morris F; ABC of clinical electrocardiography: Broad complex tachycardia - Part II. BMJ. 2002 Mar 30;324(7340):776-9.
- Weisfeldt ML, Everson-Stewart S, Sitlani C, et al; Ventricular tachyarrhythmias after cardiac arrest in public versus at home. N Engl J Med. 2011 Jan 27;364(4):313-21.
- EKG-Bibliothek
- Leitlinien für die erweiterte Erwachsenen-Ersthilfe 2021; Reanimationsrat UK
- Percutaneous (non-thoracoscopic) epicardial catheter radiofrequency ablation for ventricular tachycardia; NICE Interventional Procedure Guidance, March 2009
- Implantable cardioverter defibrillators and cardiac resynchronisation therapy for arrhythmias and heart failure; NICE Technology Appraisal Guidance, June 2014
Über den AutorVollständige Biografie anzeigen

Dr Colin Tidy, MRCGP
Allgemeinmediziner, Medizinischer Autor
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr. Colin Tidy ist ein NHS-Arzt mit Sitz in Oxfordshire.
Über den RezensentenVollständige Biografie anzeigen

Dr Hayley Willacy, FRCGP
Allgemeinmediziner, Medizinischer Autor
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr. Hayley Willacy war eine NHS-Hausärztin, die in Nordwestengland arbeitete und 2022 nach 30 Jahren aus der klinischen Praxis ausschied.
Artikelverlauf
Die Informationen auf dieser Seite wurden von qualifizierten Klinikern verfasst und begutachtet.
Artikel auch verfügbar in Englisch, Deutsch, Spanisch, Französisch, Italienisch, Portugiesisch, Hindi, Hebräisch, Arabisch, und Schwedisch.
Nächste Überprüfung fällig: 15. Okt. 2027
16. Okt 2024 | Neueste Version

Fragen, teilen, verbinden.
Durchsuchen Sie Diskussionen, stellen Sie Fragen und teilen Sie Erfahrungen zu Hunderten von Gesundheitsthemen.

Fühlen Sie sich unwohl?
Bewerten Sie Ihre Symptome online kostenlos
Mehr zu Herz-Kreislauf-Erkrankungen
- Aneurysmen und Dissektion von Arterien
- Komplikationen des akuten Myokardinfarkts
- Angeborene Herzkrankheit bei Kindern
- Dilatative Kardiomyopathien
- Schwindel, Benommenheit und Ohnmachtsgefühl
- EKG-Erkennung von Leitungsstörungen
- Endocardial fibroelastosis
- Herzabhören
- Implantierbare Kardioverter-Defibrillatoren
- Lutembacher-Syndrom
- Schmale Komplex-Tachykardien
- Nadel-Perikardiozentese
- Prävention von Herz-Kreislauf-Erkrankungen
- Prävention der infektiösen Endokarditis
- QRISK3 kardiovaskulärer Risikorechner
- Raynaud-Krankheit
- Restriktive Kardiomyopathie
- Transposition der großen Arterien
- Ventrikelseptumdefekt
- Wells-Kriterien für Lungenembolie (LE)