Bauchdeckenstraffung
Abdominoplastik
Begutachtet von Dr Helen Huins, MRCGPZuletzt aktualisiert von Dr Jacqueline Payne, FRCGPZuletzt aktualisiert 24. März 2016
Erfüllt die Anforderungen des Patienten Richtlinien des Patienten
- HerunterladenHerunterladen
- Teilen
- Language
- Diskussion
- Audio-Version
- Zu bevorzugten Quellen bei Google hinzufügen
In dieser Serie:Fettleibigkeit und GewichtsverlustGewichtszunahmeKindliche FettleibigkeitGewichtsverlustchirurgieOrlistat
Diese Seite wurde archiviert.
Es wurde kürzlich nicht überprüft und ist nicht auf dem neuesten Stand. Externe Links und Referenzen funktionieren möglicherweise nicht mehr.
Bei diesem Verfahren können überschüssige Haut und Fett entfernt, die Bauchkonturen und Narben verbessert und die Muskeln gestrafft werden.
Auf einen Blick
Abdominoplasty is a surgical procedure to remove excess skin and fat from the abdomen.
There are different types of abdominoplasty, including standard, mini, extended, and endoscopic.
The procedure typically leaves a long scar across the lower abdomen, sometimes with a scar around the navel.
Numbness and swelling in the lower abdomen are common after surgery.
Best results are seen in people who are a healthy weight.
You will need to stop taking the contraceptive pill and stop smoking before surgery to reduce risks.

This leaflet is provided by the Britische Vereinigung der Ästhetischen Plastischen Chirurgen, die Berufsorganisation, die für die Förderung von Bildung und Sicherheit in der ästhetischen plastischen Chirurgie verantwortlich ist.
Dies wird auch als Bauchdeckenstraffung oder Bauchstraffung bezeichnet. Verschiedene Kombinationen werden in den unterschiedlichen Verfahren kombiniert.
Die Standard-Bauchdeckenstraffung
Standard Bauchdeckenstraffung
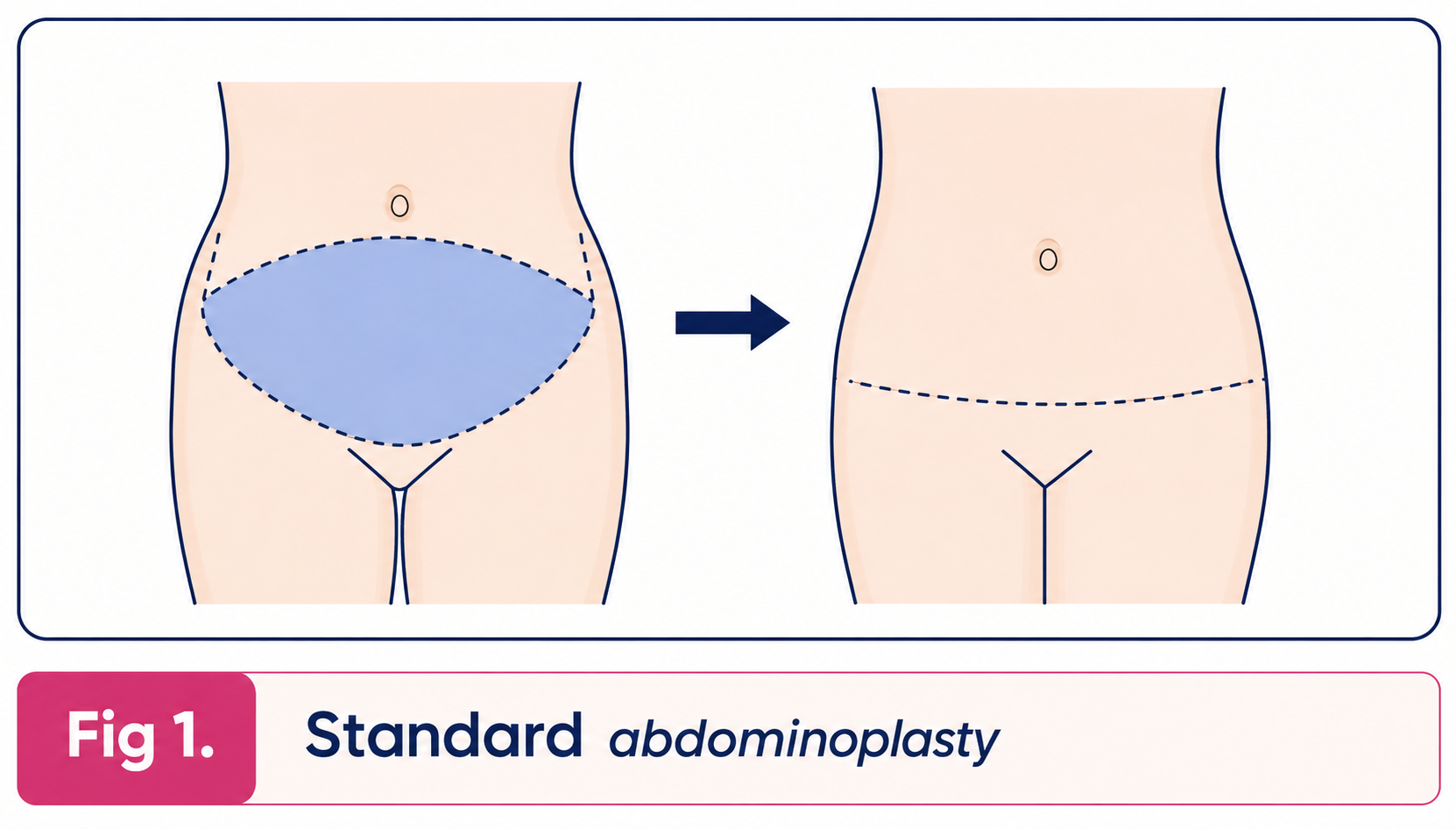
Der überschüssige Haut- und Fettgewebe der Bauchwand zwischen dem Schamhügel und dem Nabel wird entfernt, wobei der Nabel an seiner Stelle verbleibt. Die Haut der Bauchwand auf Höhe des Nabels wird nach unten gezogen und an der Schamregion vernäht. Der Patient bleibt mit einer langen, meist gebogenen Narbe im unteren Bereich der Bauchwand auf Höhe der Schamhaare zurück. Es gibt auch eine Narbe um den Nabel. Jegliche Lockerheit der Bauchmuskeln oder ein Bruch wird gleichzeitig repariert.
Fettabsaugung kann während dieses Eingriffs durchgeführt werden, um die Bauchwand zu verschmälern, oder als eigenständiger Eingriff vor oder nach der Bauchdeckenstraffung.
Mini-Bauchdeckenstraffung
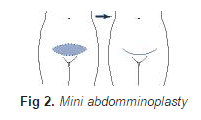
Im Mini-Bauchdeckenstraffung surplus skin below the umbilicus is removed leaving a low abdominal scar at the level of the pubic hair. The umbilicus is not disturbed but liposuction is usually carried out at the same time as the procedure to reduce the thickness of fat in the abdominal wall and any laxity or hernia of the abdominal wall is repaired at the same time.
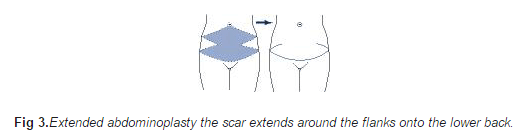
Im erweiterten Bauchdeckenstraffung surplus skin and fat of the loins and back are also removed so that the scar extends around the flanks on to the lower back.
Erweiterte Bauchdeckenstraffung
Der endoskopische Bauchdeckenstraffung is used to tighten the muscles of the abdominal wall to give a better contour and is carried out through a short transverse incision above the pubic hair. Skin is not removed but liposuction can be carried out at the same time.
Der Apronektomie is a modification of the mini-abdominoplasty for patients who have a large excess of skin and fat hanging down over the pubic area. In this procedure only the surplus skin and are removed. The scar is long and transverse extending from one side of the apron to the other.
Änderungen an der Hautentfernung bei der Bauchdeckenstraffung werden vorgenommen, wenn der Patient spezielle Probleme im Zusammenhang mit Narben früherer Operationen hat.
Ein alternatives Verfahren, das immer in Betracht gezogen werden sollte, anstelle vieler der oben genannten, ist die reine Fettabsaugung. Diese reduziert das Fett und führt nur zu einer leichten Hautstraffung.
Wer ist ein Kandidat?
Anyone who has abdominal skin and fat may be a candidate. With women the problem is usually caused by pregnancy, but is greatly aggravated by Gewichtsverlust .Die Muskeln der Bauchwand können durch Schwangerschaft geschwächt werden und sich in der Mitte tatsächlich auseinanderziehen (Rissbildung der geraden Bauchmuskeln). Männer sind ähnlich von Gewichtsverlust betroffen. Dehnungsstreifen (Striae) sind einfach die Narben, die nach extremem Dehnen der Haut verbleiben. Sie sind meist im unteren Bereich der Bauchwand am deutlichsten sichtbar. Es gibt keine spezielle Behandlung für diese Dehnungsstreifen, aber viele werden bei einer Bauchdeckenstraffung entfernt, und die verbleibenden werden gestrafft, sodass sie weniger auffällig aussehen.
Patienten, die die Haut der Bauchwand durch Bewegung nicht straffen können oder einen glatteren, flacheren Bauch erreichen möchten, profitieren ebenfalls.
Was sind die Konsequenzen?
Der Patient bleibt mit sichtbaren Narben zurück. Die Hauptnarbe verläuft quer über den unteren Bauchbereich (siehe Abbildungen oben), und bei einer Standard-Bauchdeckenstraffung wird eine Narbe um den Bauchnabel entstehen. Andere oder unterschiedliche Narben können an Stellen verbleiben, die bei individuellen Problemen des Patienten auftreten. Manche Patienten hinterlassen bessere Narben als andere, und in jedem Fall sind alle Narben anfangs rot. Es ist wichtig, dass der Patient versteht, wo diese Narben sein werden, und sie mit dem Chirurgen bespricht. Obwohl wir versuchen, sie unter Unterwäsche und Badebekleidung zu verbergen, können Modetrends ändern, sodass zuvor verdeckte Narben sichtbar werden.
Es besteht Taubheit im unteren Bereich der Bauchwand nach der Operation. Dies ist in der Regel vorübergehend, kann aber dauerhaft sein. Über dem Narbenbereich ist normalerweise eine Schwellung vorhanden, die durch eine Ansammlung von Gewebsflüssigkeit verursacht wird und normalerweise in die Leistengegend abfließt. Diese Schwellung oder Ödem klingt innerhalb weniger Monate ab.
Was sind die Einschränkungen?
Die Haut wird in der Regel nach unten gestrafft, wodurch die Taille nicht gestrafft wird. Wenn dies gewünscht ist, kann man eine vertikale Hautentfernung in Betracht ziehen, aber man sollte bedenken, dass vertikale Narben am Bauch weniger schön sind. Das Gewebe der Bauchwand ist in der Regel dicker als die Leistengegend, und wenn keine Liposuktion durchgeführt wird, kann oberhalb der Narbe eine Fettwulst verbleiben.
Die positiven Effekte der Operation werden lange anhalten. Allerdings werden die Ergebnisse besser erhalten bleiben, wenn der Patient die Muskeln weiterhin trainiert und das Gewicht stabil hält. Eine weitere Schwangerschaft wird die Haut natürlich wieder dehnen, wahrscheinlich jedoch nicht in gleichem Maße.
Was sind die Risiken?
Die Standard-Abdominoplastik ist ein großer Eingriff, der eine stationäre Behandlung von zwei bis vier Tagen erfordert. Drainagen werden entfernt, wenn sie nach einigen Tagen nach dem Eingriff kein Blut und Serum mehr ablassen. Diese Flüssigkeit kann sich nach Entfernung der Drainagen wieder ansammeln und erfordert eine Ableitung oder Aspiration.
Healing can be slow particularly in the tighter central part of the wound and sometimes dressings are needed for a few weeks. This is more common in patients who are overweight und rauchen. Dies neigt dazu, auffälligere Narben zu hinterlassen, die verbunden sind – diese können überarbeitet werden.
Secondary procedures are sometimes carried out to tidy up the results and will involve scar revision and limited liposuction. Displacement of the umbilicus to one side has been over-publicised and is rare. Tiefe Venenthrombose und Lungenembolie are rare complications of any operation, including this one.
Was müssten Sie vor der Operation tun?
Wenn Sie Übergewicht haben, ist es ratsam, eine Diät zu machen, da die besten Ergebnisse bei Menschen erzielt werden, die das richtige Gewicht für ihre Größe haben. Wenn Sie die Antibabypille nehmen, sollten Sie diese sechs Wochen vor der Operation absetzen und eine alternative Methode verwenden, um das Risiko einer Thrombose zu verringern. Wenn Sie rauchen, besteht ein größeres Risiko für eine Lungeninfektion, und insbesondere die Heilung der Bauchwunde ist weniger gut.
Was Sie bei der Operation erwarten sollten
Sie müssen ein bis drei Tage im Krankenhaus bleiben. Wenn Sie nach Ihrer Operation aufwachen, ist es wahrscheinlich, dass Sie eine Salzlösung-Transfusion erhalten. Das ist ganz normal und soll Ihnen die Flüssigkeit zuführen, die Sie brauchen, während Sie nichts trinken. Wahrscheinlich werden Drainageröhren auf beiden Seiten des unteren Bauches herauskommen, um Blut- oder Serumansammlungen abzuleiten. Sie können mit mäßig starken Schmerzen rechnen, für die Ihnen Schmerztabletten oder -spritzen verabreicht werden. Sie werden gebeten, Ihre Knie und Hüften gebeugt zu halten, um den Zug auf Ihre Nähte zu verringern.
Erholung
Übermäßige Aktivität in den ersten Tagen verringert die Heilung und erhöht die Flüssigkeitsansammlung. Leichte Aktivitäten sind nach 10 bis 20 Tagen angenehm. Sport ist etwa 6 Wochen lang nicht möglich, insbesondere wenn die Muskeln mit Nähten gestärkt wurden. Ein Korsett ist in der Regel hilfreich, um die Schwellung zu reduzieren und den Komfort im ersten Monat zu verbessern.
Content used with permission from the British Association of Aesthetic Plastic Surgeons website: Bauchdeckenstraffung (Abdominoplastik). Das Urheberrecht für dieses Informationsblatt liegt bei der BAAPS.
Haftungsausschluss
Dieses Informationsblatt soll nützliche Informationen liefern, ist jedoch nicht als spezifische Beratung für einen bestimmten Fall zu betrachten. Es ersetzt nicht die Notwendigkeit einer gründlichen Beratung, und alle potenziellen Patienten sollten den Rat eines entsprechend qualifizierten Arztes einholen. Die BAAPS übernimmt keine Haftung für Entscheidungen, die der Leser in Bezug auf die Behandlung trifft, die er durchzuführen beabsichtigt.
Patientenauswahl für Andere Operationen und Verfahren

Chirurgie und Verfahren
Vasektomie
Die Vasektomie ist eine Form der Empfängnisverhütung, bei der ein Mann eine kleine Operation durchführt, um das Ende des Samenleiters zu durchtrennen. Dies ist der Kanal, der die Spermien von den Hoden (Testes) zum Penis transportiert. Spermien werden in den Hoden produziert. Sobald der Samenleiter durchtrennt ist, können die Spermien nicht mehr in das Ejakulat gelangen, das beim Geschlechtsverkehr austritt. Die Vasektomie ist sehr zuverlässig – aber nicht zu 100 %. Selbst nach einer erfolgreichen Operation werden etwa 1 von 2.500 Männern, die eine Vasektomie hatten, irgendwann wieder fruchtbar. Dies liegt daran, dass sich die beiden Enden des durchtrennten Samenleiters selten im Laufe der Zeit wieder verbinden.
von Dr. Philippa Vincent, MRCGP

Chirurgie und Verfahren
Chirurgische Drainagen
Ein chirurgischer Drain ist ein kleines Plastikrohr, das nach einer Operation manchmal verwendet wird. Es wird während der Operation vom Arzt in Ihren Körper eingeführt und ragt bis zur Entfernung aus Ihrem Körper heraus, in der Regel nach einigen Tagen. Es ist mit einem kleinen Plastikbeutel verbunden, der Flüssigkeit oder Luft auffängt, die sich an der Operationsstelle abgelassen haben. Nicht alle Operationen erfordern einen Drain: Ihr Chirurg wird Sie darüber informieren, ob einer notwendig ist.
von Dr. Rachel Hudson, MRCGP
Häufig gestellte Fragen
What is an apronectomy, and how is it different from other abdominoplasty procedures?
An apronectomy is a specific type of abdominoplasty designed for patients with a significant excess of skin and fat that hangs down over the pubic area, often referred to as an 'apron.' Unlike some other procedures, it solely focuses on removing this surplus skin and fat, leaving a long, transverse scar from one side of the apron to the other. It doesn't involve repositioning the navel or extensive muscle tightening in the same way a standard abdominoplasty might.
Can abdominoplasty completely remove all my stretch marks?
Abdominoplasty primarily focuses on removing excess skin and fat. While many stretch marks, particularly those on the lower part of the abdominal wall, may be excised along with the skin, some might remain. The remaining stretch marks will be tightened due to the skin reduction, which can make them appear less obvious, but there is no specific treatment for stretch marks themselves.
Will an abdominoplasty help me achieve a tighter waist?
Generally, an abdominoplasty primarily tightens the skin downwards on the abdomen, which typically does not tighten the waist. If tightening the waist is a specific goal, alternative approaches might need to be considered, such as removing skin vertically. However, it's important to note that vertical abdominal scars tend to be less aesthetically pleasing than horizontal ones.
How long will I experience numbness after the surgery?
Numbness in the lower part of the abdominal wall is common after abdominoplasty. This condition is usually temporary, meaning it should resolve over time. However, in some cases, the numbness could become permanent.
What can I do to ensure the best long-term results from my abdominoplasty?
To best maintain the beneficial effects of an abdominoplasty, it is important to continue exercising your abdominal muscles and keep your weight stable. While the procedure's effects are generally lasting, significant weight fluctuations or further pregnancies can stretch the skin again, though likely not to the same extent as before.
What is the typical hospital stay for a standard abdominoplasty?
A standard abdominoplasty is considered a major surgical procedure. Patients can expect to be hospitalised for two to four days following the operation.
Weiterführende Literatur und Referenzen
- Calle EE, Rodriguez C, Walker-Thurmond K. u.a; Übergewicht, Fettleibigkeit und die Sterblichkeit durch Krebs in einer prospektiv untersuchten Kohorte von US-amerikanischen Erwachsenen. N Engl J Med. 2003 Apr 24;348(17):1625-38.
- Flegal KM, Kit BK, Orpana H, et al; Zusammenhang zwischen der Gesamtmortalität und Übergewicht sowie Fettleibigkeit anhand standardisierter Body-Mass-Index-Kategorien: eine systematische Übersicht und Meta-Analyse. JAMA. 2013 Jan 2;309(1):71-82. doi: 10.1001/jama.2012.113905.
- Fettleibigkeit im Vereinigten Königreich: Eine psychologische Perspektive; British Psychological Society, 2011
- Übergewicht und Fettleibigkeit im Kindesalter; Weltgesundheitsorganisation
- Oude Luttikhuis H, Baur L, Jansen H, et al; Intervention bei der Behandlung von Fettleibigkeit bei Kindern. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD001872. doi: 10.1002/14651858.CD001872.pub2.
- MEND; (Geist, Bewegung, Ernährung ... Mach es!)
- Positionsaussage: Kinderübergewicht; Royal College of Paediatrics and Child Health, 2012
- Hsia DS, Fallon SC, Brandt ML; Adoleszenten-Bariatrische Chirurgie. Arch Pediatr Adolesc Med. 2012 Aug;166(8):757-66. doi: 10.1001/archpediatrics.2012.1011.
- Sjostrom L; Übersicht über die wichtigsten Ergebnisse der schwedischen Obesitas-Studie (SOS) - eine prospektive kontrollierte Interventionsstudie zur bariatrischen Chirurgie. J Intern Med. 2013 Mär;273(3):219-34. doi: 10.1111/joim.12012. Epub 2013 Feb 8.
- Gesundes Leben, gesunde Menschen. Ein Aufruf zum Handeln gegen Fettleibigkeit in England; Gesundheitsministerium, 13. Oktober 2011
- Fettleibigkeit reduzieren und Ernährung verbessern: Politik; Gesundheitsministerium, März 2013
- Körpermasseindex (BMI) Diagramme für Mädchen und Jungen im Alter von 2-18 Jahren; Königliches Kollegium für Pädiatrie und Kindergesundheit und Gesundheitsministerium
- Colquitt JL, Pickett K, Loveman E, et al; Chirurgie zur Gewichtsreduktion bei Erwachsenen. Cochrane Database Syst Rev. 2014 Aug 8;8:CD003641. doi: 10.1002/14651858.CD003641.pub4.
- Arterburn DE, Courcoulas AP; Bariatrische Chirurgie bei Fettleibigkeit und Stoffwechselerkrankungen im Erwachsenenalter. BMJ. 27. Aug. 2014;349:g3961. doi: 10.1136/bmj.g3961.
- Fettleibig, übergewichtig mit Risikofaktoren: Liraglutid (Saxenda); NICE Evidence Summary, June 2017
- Hafekost K, Lawrence D, Mitrou F, et al; Bekämpfung von Übergewicht und Fettleibigkeit: Entspricht die Botschaft der öffentlichen Gesundheit der Wissenschaft? BMC Med. 2013 Feb 18;11:41. doi: 10.1186/1741-7015-11-41.
- Über Fettleibigkeit: Body-Mass-Index; MEND - Mytime Active
- Yeh JS, Kushner RF, Schiff GD; Fettleibigkeit und Management der Gewichtsabnahme. N Engl J Med. 2016 Sep 22;375(12):1187-9. doi: 10.1056/NEJMclde1515935.
Über den AutorVollständige Biografie anzeigen

Dr Jacqueline Payne, FRCGP
Allgemeinmediziner, Medizinischer Autor
MB, BS, DFFP, DRCOG, FRCGP
Jacqueline war 25 Jahre lang Hausärztin in Kendal, Cumbria, wo sie junge Hausärzte für das RCGP ausbildete und als Ausbilderin für das FSRH tätig war.
Über den RezensentenVollständige Biografie anzeigen

Dr Helen Huins, MRCGP
Allgemeinmediziner, Medizinischer Autor
MB, BS, Lond, DCH, DRCOG, MRCGP, JCPTGP, DFFP
Helen qualified at Guy’s Hospital in 1989 and left London in 1990 to settle in the countryside.
Artikelverlauf
Die Informationen auf dieser Seite wurden von qualifizierten Klinikern verfasst und begutachtet.
Artikel auch verfügbar in Englisch, Deutsch, Spanisch, Französisch, Italienisch, Portugiesisch, Hindi, Hebräisch, Arabisch, und Schwedisch.
24. März 2016 | Neueste Version

Fragen, teilen, verbinden.
Durchsuchen Sie Diskussionen, stellen Sie Fragen und teilen Sie Erfahrungen zu Hunderten von Gesundheitsthemen.

Fühlen Sie sich unwohl?
Bewerten Sie Ihre Symptome online kostenlos
Abonnieren Sie den Patienten-Newsletter
Ihre wöchentliche Dosis klarer, vertrauenswürdiger Gesundheitsberatung - geschrieben, um Ihnen zu helfen, sich informiert, selbstbewusst und in Kontrolle zu fühlen.
Durch das Abonnieren akzeptieren Sie unsere Datenschutzrichtlinie. Sie können sich jederzeit abmelden. Wir verkaufen Ihre Daten niemals.
Mehr zu Chirurgie und Verfahren
- Anästhesie
- Anästhesie für Hüft- oder Kniegelenkersatz
- Arthroskopie und arthroskopische Chirurgie
- Biopsie
- Knochenmarkbiopsie und Aspiration
- Brustvergrößerung
- Brustverkleinerung
- Koronarangioplastie
- Koronararterien-Bypass-Operation
- Endobronchialer ultraschallgesteuerter transbronchialer Nadelaspiration
- Epidurale Schmerzbehandlung nach der Operation
- Gastroskopie
- Hüftgelenkersatz
- Kniegelenkersatz
- Laser-Haarentfernung
- Lokalanästhesie für Ihre Augenoperation
- Nasenverkleinerung (Rhinoplastik)
- Kopfschmerzen nach duraler Punktion
- Postoperative Brustinfektion
- Spinalanästhesie