Knöchelverletzungen und Verstauchungen
Begutachtet von Dr Laurence KnottZuletzt aktualisiert von Dr Colin Tidy, MRCGPZuletzt aktualisiert 15. Feb 2022
Erfüllt die Anforderungen des Patienten redaktionellen Richtlinien
- HerunterladenHerunterladen
- Teilen
- Language
- Diskussion
- Audio-Version
- Zu bevorzugten Quellen bei Google hinzufügen
Medizinische Fachkräfte
Fachartikel sind für die Nutzung durch Gesundheitsfachkräfte konzipiert. Sie werden von britischen Ärzten verfasst und basieren auf Forschungsergebnissen sowie britischen und europäischen Richtlinien. Sie finden möglicherweise die Knöchelverletzung Artikel nützlicher oder einer unserer anderen Gesundheitsartikel.
Siehe auch das separate Ankle Fractures Artikel.
Ankle sprains and injuries are common in primary care, A&E and sports medicine1 . Most are inversion and plantar flexion injuries that lead to damage to the lateral ligaments2 .
The ankle is a complex joint which is capable of a wide range of movement: flexion, extension, inversion and eversion as well as a combination of these movements. This allows locomotion and balance on both level and uneven ground. The ankle takes the full weight of the body and is subject to considerable force, particularly in running and jumping.
Many ankle injuries are managed conservatively. However, obvious clinical deformity (ie dislocation) or injuries with neurovascular compromise of the foot are an orthopaedic emergency for which immediate reduction is required (see 'Management' section, below).
Between 50% and 70% of people who sustain a lateral ankle sprain will develop chronic ankle instability, which is characterised by lingering pain, instability, injury recurrence, and persistent functional disability3 .
Anatomie des Sprunggelenks2
Zwei Gelenke ermöglichen die Bewegung des Knöchels:
Das eigentliche Sprunggelenk (tibiotalar Gelenk) - die Artikulation erfolgt zwischen dem unteren Ende der Tibia, den Malleolen und dem Körper des Talus. Dieses Gelenk ermöglicht die Dorsalflexion und Plantarflexion des Sprunggelenks.
Das subtalare Gelenk - die Artikulation erfolgt zwischen dem Talus und dem Calcaneus. Dieses Gelenk ermöglicht die Inversion und Eversion des Knöchels.
Die distale Tibia hat einen prominenten medialen Malleolus und einen weniger prominenten posterioren Malleolus. Die distale Fibula ist als lateraler Malleolus bekannt. Die Gelenkkapsel und die umliegenden Bänder stabilisieren das Sprunggelenk. Die distale Fibula ist durch die vorderen und hinteren unteren tibiofibularen Bänder, ein unteres transversales Band und ein Syndesmosenband mit der distalen Tibia verbunden. Die vorderen und hinteren talofibularen Bänder verbinden die Fibula mit dem Talus. Der Talus ist durch das calcaneo-fibulare Band mit dem Calcaneus verbunden. Das Deltaband verbindet den medialen Malleolus mit dem Talus, Calcaneus und den Navicularknochen.
Gelenke des Knöchels und Fußes
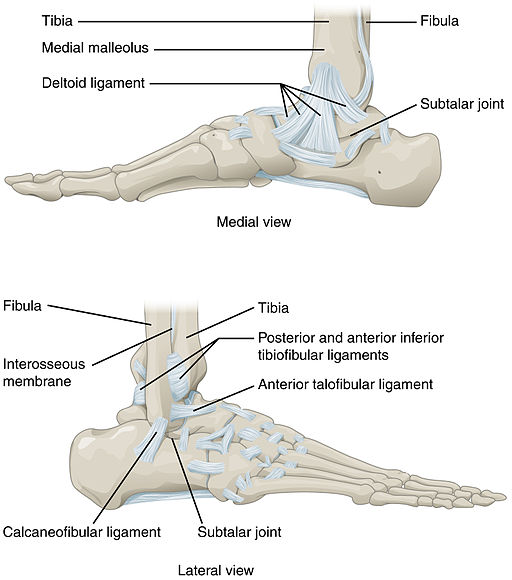
© OpenStax College, Anatomie & Physiologie, Connexions-Website, 19. Juni 2013, über Wikimedia Commons
Assessment of ankle injuries4
Initial assessment should follow the principles for any trauma:
Carry out a primary survey following the 'ABCDE' principles of resuscitation and trauma care.
Assess clinically for obvious deformity and for neurovascular status. If there is neurovascular compromise or dislocation (obvious deformity) of the joint, the fracture should be reduced immediately under analgesia or sedation.
Verschobene Frakturen sollten so schnell wie möglich nach der Erstuntersuchung reponiert werden - dies reduziert Schmerzen/Schwellungen und kann Hautnekrosen verhindern.
History and examination help to decide whether there has been a significant likelihood of an ankle fracture or foot fracture. Apply and document the Ottawa Rules5 6 .
Anamnese
Ask how long ago the ankle injury occurred.
Mechanism of injury: injuries are most often whilst crossing uneven ground or after a sudden change of direction whilst playing sport:
Was there excessive inversion or eversion? The injury may have resulted from jumping from a height.
Was there a 'snap' sound? (This does not differentiate between a sprain and a fracture2 .)
Where is the pain felt?
Was geschah danach? Konnte der Patient sofort Gewicht tragen? Brauchten sie Hilfe beim Gehen? Wenn es eine Sportverletzung war, konnten sie weitermachen?
Was there immediate swelling? (Immediate swelling is due to bleeding and suggests significant tissue injury.)
Previous ankle injury: establish whether there is underlying weakness or instability in the ankle and whether an old fracture might be evident on X-ray.
Past medical history - eg, osteoporosis or metabolic bone disease.
Drug history - eg, long-term corticosteroid use.
Untersuchung2
Inspection:
Note whether the patient walked in and, if they did, with how much discomfort and disability.
Look at the ankle and whether there is obvious deformity.
Note whether there is swelling or bruising and whether it looks compatible with the mechanism of injury.
Establish whether an effusion is present. This may be a fullness either side of the Achilles tendon.
Look for any open wounds.
Palpation:
Palpate for crepitus and tenderness, especially over the malleolar regions, over the anterior tibiofibular ligament, the gesamte Länge of the fibula and the base of the fifth metatarsal. Note whether calcaneal pressure elicits pain.
Examine for neurovascular injury:
Assessment of neurovascular status is by sensation over the dorsal and plantar surfaces of the foot, measuring capillary refill in all digits and palpating the distal pulses (the dorsalis pedis artery is absent in 2-3% of the population). Vascular compromise is the urgent concern in dislocations and fracture-dislocations. Sural nerve and peroneal nerve palsies are a rare complication of severe sprains.
Movement/power:
Diese können in den meisten Fällen nicht getestet werden, da das Gelenk geschwollen, schmerzhaft, gebrochen oder ausgerenkt sein kann.
Examine for co-existing injuries:
Achten Sie besonders auf das ipsilaterale Knie und den Fuß.
Überprüfen Sie auf Druckempfindlichkeit (Fraktur) des proximalen Wadenbeins.
Specific tests (if appropriate and tolerable to the patient) include:
Thompson's test: this is to assess if the Achilles tendon is intact. With the patient lying prone with the knee flexed to 90°, squeeze the posterior calf muscles - this should produce a visible plantar flexion at the ankle if the tendon is intact.
The anterior drawer test: this can show excessive anterior displacement of the talus on to the tibia. If the anterior talofibular ligament is torn, the talus will subluxate anteriorly compared with the unaffected ankle. With the ankle in a neutral position, stabilise the leg over the distal tibia with one hand and cup the heel with the other, pulling the foot forward. The patient should be relaxed and both legs compared. A positive sign is a greater anterior movement on the injured side, with the injured side having more movement than the uninjured.
The talar tilt test (also called the inversion stress test): this stresses the calcaneo-fibular ligament. This test is not usually feasible in acute injuries, owing to swelling; however, it may be used to assess stability during healing. With the foot in a neutral position, hold the lower leg in one hand and the heel in the other: invert the ankle. Compare with the other leg.
Tests for syndesmosis injury:
Squeeze test: involves squeezing the tibia and fibula together at the mid calf. If pain is experienced more distally or in the ankle, this is a positive test.
Interosseous membrane tenderness test: this also looks for syndesmosis injury. Position the patient supine. Palpate between the tibia and fibular from the ankle proximally. Note the length of tenderness.
External rotation stress test: externally rotate and then passively dorsiflex the ankle. Pain at the syndesmosis is a positive test.
Die Untersuchung des unverletzten Knöchels kann einen Hinweis auf den normalen Bewegungsumfang und die Kraft geben.
Untersuchungen
The first question is often how to rule out ankle fracture, particularly where there is difficulty in weight bearing.
Ankle X-rays: Ottawa Rules6 7
Clinically it may be very difficult to differentiate a fracture from a severe sprain without an X-ray unless there is obvious distortion or instability. The Ottawa Ankle Rules were introduced in 1992 as a guideline with which to reduce costs and waiting times when ruling out serious ankle and midfoot fractures in the non-athletic, adult population.
Eine Röntgenaufnahme des Knöchels ist nur angezeigt, wenn ein Patient Schmerzen im Malleolarbereich hat und eines der folgenden Symptome vorliegt:
Knochendruckschmerz am hinteren Rand oder an der Spitze des medialen oder lateralen Malleolus, oder
Unfähigkeit, Gewicht zu tragen (vier Schritte) unmittelbar nach der Verletzung und zum Zeitpunkt der Beurteilung.
Eine Röntgenaufnahme des Fußes ist nur angezeigt, wenn ein Patient Schmerzen im Mittelfußbereich hat und eines der folgenden Symptome vorliegt:
Bone tenderness at the base of the fifth metatarsal or over the navicular bone (located on the top inner side of the middle of the foot) or
Unfähigkeit, Gewicht zu tragen (vier Schritte) unmittelbar nach der Verletzung und zum Zeitpunkt der Beurteilung.
Die Buffalo-Regel wurde entwickelt, um die diagnostische Genauigkeit der Ottawa-Knöchel-Regeln zu erhöhen, wobei das Kriterium der Druckempfindlichkeit auf den Kamm oder den mittleren Teil der Malleolen (distale 6 cm der Fibula und Tibia) gerichtet ist, wodurch die Wahrscheinlichkeit verringert wird, über verletzte Bandstrukturen zu palpieren7 .
Assessment of the Ottawa Ankle Rules suggests that they are valid in children, and they are in widespread clinical use, as they massively reduce costs and unnecessary X-ray exposure8 .
Bildgebung
If an X-ray is performed, anteroposterior (AP), lateral and mortise views can be taken. For the mortise view, the foot is rotated about 15° internally. This allows a better view of the ankle mortise.
Wenn auf dem Röntgenbild eine Verletzung zu sehen ist, suchen Sie immer nach einer zweiten.
CT and MRI scanning are sometimes needed for fracture diagnosis and assessment of ligamentous or intra-articular injuries.
Ankle fracture diagnosis
The diagnosis and management of ankle fracture is covered in the separate Ankle Fractures Artikel.
Ankle sprain diagnosis9
The ankle and knee are commonly affected.
The severity of symptoms and signs depends on the severity of the sprain (for example, whether there has been a partial or complete ligament tear). Common symptoms and signs include:
Schmerzhaftigkeit und Schwellung.
Blutergüsse.
Functional loss (for example, pain on weight-bearing).
Mechanical instability (if the sprain is severe).
Marked bruising and swelling, which may indicate a complete ligament tear or fracture.
Ankle muscle strain diagnosis9
There is commonly confusion between the terms sprain and strain. A Anstrengung includes inflammation of muscles and tendons. A sprain is a ligament injury.
The clinical features of a muscle strain depend on the severity of the injury and the nature of the haematoma.
There may be a history of a strain or 'pulled muscle'.
Pain occurs in the affected muscle.
Large haematomas can occur as a result of tearing of the intramuscular blood vessels.
There may be obvious swelling, although small haematomas or those deep within the muscle are more difficult to diagnose clinically.
Muscle function may be affected, depending on the severity of the strain.
Differentialdiagnose
Commonly missed ankle/foot fractures are2 :
Proximal fibula.
Base of fifth metatarsal (also a common site for stress fractures).
Talus - dome, lateral process (Snowboarder's fracture) or posterior process.
Tibial plafond.
Other causes of acute ankle pain are:
Joint pathology - eg, Gicht, osteochondritis dissecans.
Tendon injury - eg, flexor hallucis longus, posterior tibialis or anterior tibialis tendon injuries; peroneal tendon subluxation.
Anterior process fracture of the calcaneus.
Ankle sprains - classification2
Lateral ankle sprains
These account for 85% of all ankle sprains, most commonly due to inversion of the plantar flexed foot10 .
Ankle sprains are classified from grade I to grade III depending on their severity:
Grade I injuries - the ligament is stretched, with microscopic (but not macroscopic) tearing. Swelling is mild, with little or no functional loss and no joint instability. The patient bears weight at least partially.
Grade II injuries - the ligament is stretched with partial tearing. Swelling is moderate-to-severe, with ecchymosis.There is moderate functional loss and mild-to-moderate joint instability. Patients usually have difficulty bearing weight.
Grade III injuries - the ligament is completely ruptured. Swelling is immediate and severe, with ecchymosis. The patient usually cannot bear weight (or not without severe pain). There is moderate-to-severe instability of the joint.
Syndesmotic (high ankle) sprain
This is caused by dorsiflexion and eversion of the ankle with internal rotation of the tibia - eg, during skiing or football. The syndesmotic ligaments are the combination of the interosseous ligament and lower tibiofibular ligaments which normally stabilise the mortise joint and fix the fibula in the fibular notch.
Look for widening of the mortise (tibiofibular gap should be <5 mm measured 1 cm above the joint line on AP and mortise views).
Squeeze test, side-to-side test and forced external rotation all cause pain at the syndesmosis.
Healing takes longer than standard lateral sprains - consider the diagnosis in those with continuing pain more than six weeks after the original injury.
Treatment and management of ankle sprains9 10 11
Treatment aim is to minimise discomfort and restore function. Most ligament injuries heal well, although there may be scarring.
Functional support is generally preferable to immobilisation, unless the injury is severe. This means the use of a variable or immovable immobilising device in conjunction with exercise.
Lateral sprains are most common and can be treated conservatively.
Simple medial sprains can also be treated conservatively but tenderness over the deltoid ligament, with or without laxity, associated with fractures or instability, may require fixation.
One overview of systematic reviews found that12 :
For the treatment of acute ankle sprain, there is strong evidence for non-steroidal anti-inflammatory drugs and early mobilisation, with moderate evidence supporting exercise and manual therapy techniques, for pain, swelling and function.
Exercise therapy and bracing are supported in the prevention of chronic ankle instability.
Treatment for the first 72 hours
Protection, rest, ice, compression and elevation (PRICE)
Protect from further injury (for example, by a tubular support bandage, ankle tape, brace or high-top high-lace shoes 13 ).
Rest the ankle joint for 48-72 hours following injury. Consider the use of crutches in this period. In most cases, early controlled weight-bearing with the ankle well supported is preferable to complete rest.
Wce should be applied as soon as possible after injury, for 10-30 minutes. (Less than 10 minutes has little effect. More than 30 minutes may damage the skin.) Do not put ice directly next to skin, as it may cause ice burn. This may limit pain, inflammation and bruising. Some doctors recommend re-applying for 15 minutes every two hours (during daytime) for the first 48-72 hours. Do not leave ice on while asleep.
Compression with a bandage will limit swelling.
Elevation aims to limit and reduce any swelling.
Avoidance of heat, alcohol, running and massage (HARM)
Heat - which encourages blood flow which will tend to increase bruising and inflammation.
Alcohol, which can increase bleeding and swelling and decrease healing.
Running, which may cause further damage.
Massage, which may increase bleeding and swelling.
Other treatment
Analgesia if required.
For simple sprains which are not severe, begin flexibility (range of motion) exercises as soon as they can be tolerated without excessive pain.
For severe sprains (type III) a short period of immobilisation can result in quicker recovery. A short period of immobilisation in a below-knee cast or pneumatic brace may speed recovery compared to a compression bandage alone14 15 .
Treatment of syndesmotic sprains may involve a fracture boot, short leg cast or non-weight bearing. Internal fixation may be required if the joint is unstable. See the separate Ankle Fractures Artikel.
Rarely, if ligaments are badly torn or the joint unstable, surgical repair may be indicated.
Physiotherapy may be helpful in restoration to a full range of normal movement, improving the strength of the surrounding muscles and improving proprioception.
Avoidance of sport or vigorous exercise involving the ankle for at least 3-4 weeks after a sprain.
Rehabilitation after ankle sprain
After injury, full rehabilitation to build up the muscles around the joint is important; weak muscles can predispose to further injury. Guided rehabilitation over a period of weeks is recommended2 .
Athletes with severe sprains may need an ankle orthosis for several months following the injury2 .
Chronic ankle instability may follow an acute lateral ankle sprain. Initial treatment involves bracing or neuromuscular training. However, if symptoms persist, surgery may be considered16 .
After a sprain, persistent symptoms remain in up to 30% of individuals10 .
Prevention of ankle sprain
Prevention of ankle sprains may be facilitated by wearing walking boots that protect the ankle (rather than shoes) when hiking over hills or uneven ground, or for manual labour.
Management of muscle strain
Immobilise the injured muscle for the first few days after the injury. Consider the use of crutches in severe injuries.
Start active mobilisation after a few days if the person has pain-free use of the muscle in basic movements and the injured muscle can stretch as much as the healthy contralateral muscle.
Dr. Mary Lowth ist eine Autorin oder die ursprüngliche Autorin dieses Merkblatts.
Exklusive Updates für medizinisches Fachpersonal
Bleiben Sie informiert mit den neuesten klinischen Updates, professionellen Einblicken und evidenzbasierten Leitlinien. Der Patient Pro-Newsletter stellt wesentliche Inhalte für Gesundheitsfachkräfte zusammen – direkt in Ihren Posteingang geliefert.
Durch das Abonnieren akzeptieren Sie unsere Datenschutzrichtlinie. Sie können sich jederzeit abmelden. Wir verkaufen Ihre Daten niemals.
Weiterführende Literatur und Referenzen
- Suture fixation of acute disruption of the distal tibiofibular syndesmosis; NICE Leitlinie für interventionelle Verfahren, Juni 2015
- Tiemstra JD; Aktualisierung zu akuten Knöchelverstauchungen. Am Fam Physician. 15. Juni 2012;85(12):1170-6.
- D'Hooghe P, Cruz F, Alkhelaifi K; Return to Play After a Lateral Ligament Ankle Sprain. Curr Rev Musculoskelet Med. 2020 Jun;13(3):281-288. doi: 10.1007/s12178-020-09631-1.
- Herzog MM, Kerr ZY, Marshall SW, et al; Epidemiology of Ankle Sprains and Chronic Ankle Instability. J Athl Train. 2019 Jun;54(6):603-610. doi: 10.4085/1062-6050-447-17. Epub 2019 May 28.
- Slimmon D, Brukner P; Sportknöchelverletzungen - Bewertung und Management. Aust Fam Physician. 2010 Jan-Feb;39(1-2):18-22.
- Gribble PA; Evaluating and Differentiating Ankle Instability. J Athl Train. 2019 Jun;54(6):617-627. doi: 10.4085/1062-6050-484-17. Epub 2019 Jun 4.
- Lynch SA; Beurteilung des verletzten Knöchels bei Sportlern. J Athl Train. 2002 Dez;37(4):406-412.
- Ankle Injury - X-ray for Acute Injury of the Ankle or Mid-Foot: Ottawa Rules reiterated; British Columbia Canada
- Ottawa Ankle Rules; Ottawa Hospital, Canada
- Jenkin M, Sitler MR, Kelly JD; Klinische Nützlichkeit der Ottawa-Knöchel-Regeln zur Erkennung von Frakturen des Knöchels und Mittelfußes. J Athl Train. 2010 Sep-Okt;45(5):480-2. doi: 10.4085/1062-6050-45.5.480.
- Bulloch B, Neto G, Plint A, et al; Validierung der Ottawa-Knie-Regel bei Kindern: eine multizentrische Studie. Ann Emerg Med. 2003 Jul;42(1):48-55.
- Verstauchungen und Zerrungen; NICE CKS, April 2020 (nur für UK-Zugang)
- Lin CW, Hiller CE, de Bie RA; Evidence-based treatment for ankle injuries: a clinical perspective. J Man Manip Ther. 2010 Mar;18(1):22-8.
- Halabchi F, Hassabi M; Acute ankle sprain in athletes: Clinical aspects and algorithmic approach. World J Orthop. 2020 Dec 18;11(12):534-558. doi: 10.5312/wjo.v11.i12.534. eCollection 2020 Dec 18.
- Doherty C, Bleakley C, Delahunt E, et al; Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med. 2017 Jan;51(2):113-125. doi: 10.1136/bjsports-2016-096178. Epub 2016 Oct 8.
- Kemler E, van de Port I, Backx F, et al; A systematic review on the treatment of acute ankle sprain: brace versus other functional treatment types. Sports Med. 2011 Mar 1;41(3):185-97.
- Seah R, Mani-Babu S; Managing ankle sprains in primary care: what is best practice? A systematic Br Med Bull. 2011;97:105-35. Epub 2010 Aug 14.
- Lamb SE, Marsh JL, Hutton JL, et al; Mechanical supports for acute, severe ankle sprain: a pragmatic, multicentre, randomised controlled trial. Lancet. 2009 Feb 14;373(9663):575-81.
- de Vries JS, Krips R, Sierevelt IN, et al; Interventions for treating chronic ankle instability. Cochrane Database Syst Rev. 2011 Aug 10;(8):CD004124.
Über den AutorVollständige Biografie anzeigen

Dr Colin Tidy, MRCGP
Allgemeinmediziner, Medizinischer Autor
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr. Colin Tidy ist ein NHS-Arzt mit Sitz in Oxfordshire.
Über den RezensentenVollständige Biografie anzeigen

Dr. Laurence Knott
Allgemeinmediziner, Medizinischer Autor
BSc (Hons) Biochemie, MBBS
Dr. Laurence Knott qualifizierte sich 1973 und hat umfangreiche Erfahrung als Allgemeinmediziner.
Artikelverlauf
Die Informationen auf dieser Seite wurden von qualifizierten Klinikern verfasst und begutachtet.
Artikel auch verfügbar in Englisch, Deutsch, Spanisch, Französisch, Italienisch, Portugiesisch, Hindi, Hebräisch, Arabisch, und Schwedisch.
Nächste Überprüfung fällig: 14. Feb 2027
15. Feb 2022 | Neueste Version

Fragen, teilen, verbinden.
Durchsuchen Sie Diskussionen, stellen Sie Fragen und teilen Sie Erfahrungen zu Hunderten von Gesundheitsthemen.

Fühlen Sie sich unwohl?
Bewerten Sie Ihre Symptome online kostenlos
Mehr in Orthopädie und Sportmedizin
- Schmerzende Gelenke - Beurteilung, Untersuchungen und Behandlung in der Primärversorgung
- Achondroplasie
- Knöchelbrüche
- Rückenschmerzen bei Kindern
- Blount-Krankheit
- Karpaltunnelsyndrom und Läsionen des Medianusnervs
- Kostochondritis und Tietze-Syndrom
- Crush-Syndrom
- Diffuse idiopathische Skeletthyperostose
- Ellenbogengelenkersatz
- Fragilitätsfrakturen
- Hallux rigidus
- Juvenile idiopathische Arthritis
- Verletzungen der Kniebänder
- Langerhans-Zell-Histiozytose
- Osteochondrodysplasien
- Osteochondrosen
- Osteoporose-Risikobewertung und Primärprävention
- Skoliose und Kyphose
- Kleinwuchs