Harninkontinenz
Begutachtet von Dr Philippa Vincent, MRCGPZuletzt aktualisiert von Dr Rachel Hudson, MRCGPZuletzt aktualisiert 16. Nov. 2023
Erfüllt die Anforderungen des Patienten Richtlinien des Patienten
- HerunterladenHerunterladen
- Teilen
- Language
- Diskussion
- Audio-Version
- Zu bevorzugten Quellen bei Google hinzufügen
Urinary incontinence is a common problem, affecting women more commonly than men. Belastungsinkontinenz und Dranginkontinenz are the most common types of incontinence.
Many people are embarrassed by the problem but, importantly, incontinence is often treatable so you should see your GP for help.
This leaflet provides a general overview of urinary incontinence. It may help you to understand the bladder and why incontinence occurs.
Auf einen Blick
Urinary incontinence means leaking urine unintentionally.
It is common, particularly in women, and can affect people of any age.
The two most common types are stress incontinence and urge incontinence.
Many cases of incontinence can be successfully treated or significantly improved.
See your doctor if you leak urine regularly for assessment and treatment options.
What is urinary incontinence?
If you have urinary incontinence it means that you pass urine when you do not mean to (involuntarily leaking urine). It can range from a small dribble now and then, to large floods of urine. Incontinence may cause you distress as well as being a hygiene problem.
Understanding urine and the bladder
The kidneys make urine continuously. A trickle of urine is constantly passing to the bladder down the tubes (ureters) from the kidneys to the bladder. You make different amounts of urine depending on how much you drink, eat and sweat.
Urinary tract
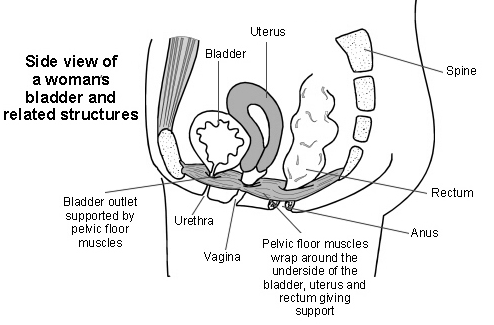
The bladder is made of muscle and stores the urine. It expands like a balloon as it fills with urine. The outlet for urine (the urethra) is normally kept closed. This is helped by the muscles below the bladder that surround and support the urethra (the pelvic floor muscles).
When a certain volume of urine is in the bladder, you become aware that the bladder is getting full. When you go to the toilet to pass urine, the bladder muscle squeezes (contracts) and the urethra and pelvic floor muscles relax to allow the urine to flow out.
Complex nerve messages are sent between the brain, the bladder and the pelvic floor muscles. These tell you how full your bladder is and tell the correct muscles to contract or relax at the right time.
How common is urinary incontinence?
Urinary incontinence is common, especially in women. It can occur at any age but it is more likely to develop as you get older. It is estimated that about three million people in the UK are regularly incontinent. Overall, this is about 4 in 100 adults. However, as many as 1 in 5 women over the age of 40 have some degree of urinary incontinence.
It is likely that the true number of people affected is much higher. Many people do not tell their doctor about their incontinence, due to embarrassment. Some people wrongly think that incontinence is a normal part of ageing or that it cannot be treated. This is unfortunate, as many cases can be successfully treated or significantly improved.
What are the causes of urinary incontinence?
Female urinary system
There are several different types of urinary incontinence:
Belastungsinkontinenz
This is the most common type of urinary incontinence. It occurs when the pressure in the bladder becomes too great for the bladder outlet to withstand. This is usually caused by weak pelvic floor muscles.
Urine tends to leak most when you cough, laugh, sneeze or exercise (such as when you jump or run). In these situations there is a sudden extra pressure (stress) inside the tummy (abdomen) and on the bladder.
Small amounts of urine often leak. Sometimes much larger volumes of urine are accidentally passed. Stress incontinence may also be a side effect of pregnancy, as pelvic floor muscles are often weakened by childbirth.
Stress incontinence is more common in women who have had several children, in obese people and with increasing age. See the separate leaflet called Stress Incontinence for more details.
Belastungsinkontinenz können occur in men who have had some treatments for Prostatakrebs. This includes surgical removal of the prostate (prostatectomy), and radiotherapy.
Urge incontinence (unstable or overactive bladder)
This is the second most common cause of urinary incontinence. You have an strong urge to urinate. Sometimes urine leaks before you have time to get to the toilet. The bladder muscle contracts too early and the normal control is reduced.
In most cases, the cause of urge incontinence is not known. This is called idiopathic urge incontinence. It seems that the bladder muscle gives wrong messages to the brain and the bladder may feel fuller than it actually is.
Sometimes urge incontinence can occur because of problems with the nervous system (the brain, spinal cord and other nerves in the body). See the separate leaflet called Urge Incontinence for more details.
Diseases or medical conditions affecting the nervous system are called neurological disorders. Some people with certain neurological disorders may experience urge incontinence. Examples are Parkinson-Krankheit, Multiple Sklerose (MS), spinal cord injury and after a Schlaganfall.
Mixed incontinence
Some people have a combination of stress and urge incontinence.
Most cases of urinary incontinence are due to the above causes. The other causes listed below are less common.
Overflow incontinence
This occurs when there is an obstruction to the outflow of urine. The obstruction prevents the normal emptying of the bladder. A pool of urine constantly remains in the bladder that cannot empty properly. This is called chronic urinary retention.
Consequently, pressure on the bladder builds up behind the obstruction. The normal bladder emptying mechanism becomes faulty and urine may leak past the blockage from time to time. Treatment depends on the cause.
Enlarged prostate urinary incontinence
An enlarged prostate gland in men is a common cause of overflow incontinence. It may be treated by surgical removal of the prostate (prostatectomy) or with medicines to shrink the prostate gland.
Bedwetting (nocturnal enuresis)
Many children - but also some adults - are affected by bedwetting.
Functional incontinence
This is the name given to urinary incontinence where there is nothing obviously wrong with the nervous system controlling the bladder and urethra, or the lower urinary tract (bladder/urethra) itself. An example would be incontinence because you were unable to reach the toilet to empty your bladder, due to poor mobility.
Other types of incontinence
These include incontinence of urine when there is a birth defect (congenital abnormality) of the urinary tract, and problems that can occur after injury, accident or during operations.
Can constipation cause urinary incontinence?
Severe long-term (chronic) constipation can stop the bladder emptying properly and cause overflow urinary incontinence (as well as stool (faecal) incontinence). Dehydration can also cause constipation.
For these reasons, try to maintain a healthy balanced diet that contains plenty of fruit, vegetables and soluble fibre. See the separate leaflets called Fibre and Fibre Supplements, Verstopfung bei Erwachsenen und Healthy Eating für weitere Details.
Testing for urinary incontinence
Urinary incontinence can often be improved and can be cured in many cases. Urinary incontinence treatment may depend on the type and cause.
Beurteilung
It is important to know which type of incontinence you have. Tell your doctor if you leak urine on a regular basis. He or she will be able to assess your symptoms, examine you and may do some simple tests to try to clarify the cause. You may also be asked to keep a diary for at least three days to assess:
How often you go to the toilet.
How much urine you pass each time.
How often you leak urine.
Sometimes a referral to a specialist is needed to clarify the type of incontinence. The sort of tests that may be done by your GP or specialist to clarify the cause include the following:
Urinanalyse
This is a simple dipstick test to check for infection, sugar (glucose), blood or protein in urine. A urinary tract infection (UTI) can cause incontinence, particularly in older people. Diabetes causes sugar in the urine and may cause increased thirst and a strong urge to urinate.
Diabetes also puts you at more risk of UTIs. Diseases of the kidney may cause blood or protein in the urine. Visible blood in the urine can be a sign of serious bladder problems or a UTI.
Residual urine
This test finds out if any urine is left in your bladder and how much urine is left, after you have gone to the toilet. The amount of urine is usually measured using an ultrasound scan which can look at your bladder and measure the amount of urine in it.
Sometimes, another method is used: a doctor or nurse may pass a thin flexible tube called a catheter into the bladder via the urine outlet (urethra). Urine then drains out to be measured.
Vaginal and anal examination
A doctor or nurse may insert a gloved finger into the vagina and back passage (rectum). This can assess the strength and tone of the pelvic floor and sphincter muscles. For men, the rectal examination can also assess the size of the prostate gland.
For women, the doctor or nurse may also look for signs of pelvic organ bulging (prolapse) during the vaginal examination. They may use an instrument called a speculum to help them with this. See the separate leaflet called Genitourinary Prolapse for more details.
Urodynamics
Dies sind tests of urine flow that are sometimes done in a hospital unit if the cause of the problem is not clear. Urodynamics may also be carried out where surgery is considered to treat the problem (see below).
Urinary incontinence treatment
Treatment depends on the type of incontinence. For example: pelvic floor exercises (also known as Kegel exercises) may cure or improve stress incontinence; bladder training may help urge incontinence; medications are sometimes used to help stop urge and stress incontinence. Occasionally an operation is performed to treat the underlying cause of incontinence, eg, to repair a vaginal prolapse, or for an enlarged prostate. Other types of incontinence are less common and treatments vary, depending on the cause. See the separate leaflets called Belastungsinkontinenz, Dranginkontinenz und Overactive Bladder Syndrome (OAB) für weitere Details.
Lifestyle changes may also significantly help some types of incontinence. These can include:
Changing how much you drink
If you drink large volumes, it follows that you will pass more urine. If you have incontinence, you should not restrict your fluid intake too much, as you risk having a lack of body fluid (dehydration).
Restricting fluids can also irritate the bladder and so make urge incontinence worse. However, if you drink excessively, moderation may improve your symptoms. Drinking 6-8 glasses of water per day is recommended by the NHS. However, there is no scientific evidence we should drink that much.
In practical terms, it is best to drink when we need to, to quench our thirst. Remember that about one fifth of the water we take every day is hidden in food and that other drinks contain water.
Changing what you drink
Drinks containing caffeine (for example, tea, coffee, hot chocolate and cola) make urge incontinence worse. This is because caffeine is a natural diuretic. Diuretics are chemicals that make you need to pass urine. If you drink a lot of caffeine-containing fluids then consider switching to decaffeinated alternatives.
Changing when you drink
You should try to maintain a normal life as much as possible with regard to drinking and visiting the toilet. However, drinking late at night may mean your sleep is disturbed by the desire to get up and go to the toilet.
Gewichtsverlust
It has been shown that losing a modest amount of weight can improve urinary incontinence in overweight and obese women. Even just 5-10% weight loss can help symptoms. If you are overweight and incontinent then you should first try to lose weight in conjunction with any other treatments.
Toilet habits
This is also dealt with in bladder training but in general it is best to visit the toilet only when you need to, rather than 'just in case'. Depending on how much (and what) you are drinking and your level of physical activity (how much you are sweating), it is normal to pass urine every 3-4 hours on average.
Überweisung zu einem Spezialisten
Your GP may advise on treatment or refer you to a continence advisor for advice on bladder training and pelvic floor exercises. Sometimes physiotherapists can help with pelvic floor exercises.
In some situations, you and your doctor may decide to wait and see how things go before trying treatment. This is because some mild cases get better on their own over time and without treatment. Sometimes a specialist (usually a urologist or a urogynaecologist if you are a woman) needs to be involved in more difficult cases.
Operation
This can be used to treat incontinence, especially stress incontinence.
Living with urinary incontinence
If your incontinence persists and is not helped by treatment, your local continence advisor can give practical advice on how to manage. They may be able to supply incontinence pants, pads and other products. These days there are many different aids, gadgets and appliances that can greatly help when living with incontinence.
Patientenauswahl für Blasenprobleme

Niere und Harnwege
Überaktives Blasensyndrom
Das Syndrom der überaktiven Blase ist sehr häufig. Symptome einer überaktiven Blase sind ein dringendes Gefühl, auf die Toilette gehen zu müssen, häufiges Wasserlassen und manchmal das Austreten von Urin, bevor man die Toilette erreicht. Die Behandlung mit Blasentraining heilt oft das Problem. Manchmal kann zusätzlich zum Blasentraining eine medikamentöse Behandlung empfohlen werden, um die Blase zu entspannen.
von Dr. Hayley Willacy, FRCGP

Niere und Harnwege
Harnverhalt
Harnverhalt bedeutet, dass Sie Probleme haben, die Blase vollständig zu entleeren. Er kann plötzlich auftreten (akuter Harnverhalt) oder sich über einen längeren Zeitraum entwickeln (chronischer Harnverhalt). Akuter Harnverhalt ist ein medizinischer Notfall. Harnverhalt tritt bei Männern häufiger auf als bei Frauen. Er wird häufiger, je älter man wird. Bei Männern in ihren 70ern tritt Harnverhalt bei etwa 1 von 100 Männern auf. Bei Männern in ihren 80ern tritt Harnverhalt bei etwa 3 von 100 Männern auf. Möglicherweise benötigen Sie Tests, um die Ursache Ihres Harnverhalts zu finden. Die Behandlung und das Ergebnis sowohl des akuten als auch des chronischen Harnverhalts hängen von der zugrunde liegenden Ursache ab. Sie sollten sofort einen Arzt aufsuchen, wenn Sie keinen Urin ablassen können, obwohl sich Ihre Blase voll und schmerzhaft anfühlt.
von Dr. Rosalyn Adleman, MRCGP
Häufig gestellte Fragen
How often should I go to the toilet if I have normal bladder function?
If you have normal bladder function, it is generally considered normal to pass urine every 3-4 hours on average. This can vary depending on how much and what you are drinking, and your level of physical activity, which affects how much you sweat.
What is functional incontinence?
Functional incontinence is when you leak urine not because there's a problem with your bladder or the nerves controlling it, but because you can't get to the toilet in time. An example would be if poor mobility prevents you from reaching the toilet when you need to empty your bladder.
Why is it important to tell my doctor about incontinence?
It is important to tell your doctor about incontinence because many cases can be successfully treated or significantly improved. Many people don't seek help due to embarrassment or because they wrongly believe it's a normal part of ageing or untreatable. Your doctor can assess your symptoms and conduct tests to determine the cause and best treatment.
What is the recommended daily fluid intake for bladder health?
While the NHS suggests 6-8 glasses of water daily, there isn't scientific evidence supporting a fixed amount. It's best to drink when you feel thirsty. Restricting fluids too much can lead to dehydration and may even irritate the bladder, potentially worsening urge incontinence. About one-fifth of our daily water intake also comes from food and other drinks.
Are there other types of incontinence besides stress, urge, and overflow?
Yes, other types include incontinence related to birth defects of the urinary tract, problems occurring after injury, accident, or operations, and bedwetting (nocturnal enuresis) affecting both children and some adults. Functional incontinence, where physical inability to reach the toilet is the cause, is another type.
Weiterführende Literatur und Referenzen
- Thirugnanasothy S; Managing urinary incontinence in older people. BMJ. 2010 Aug 9;341:c3835. doi: 10.1136/bmj.c3835.
- Wing RR, Creasman JM, West DS, et al; Improving urinary incontinence in overweight and obese women through modest weight loss. Obstet Gynecol. 2010 Aug;116(2 Pt 1):284-92.
- Urinary incontinence in neurological disease: assessment and management; NICE Clinical Guideline (August 2012 - last updated October 2023)
- Harninkontinenz und Beckenorganprolaps bei Frauen: Behandlung; NICE-Richtlinie (April 2019 - aktualisiert Juni 2019)
- Inkontinenz - Harninkontinenz bei Frauen; NICE CKS, Juli 2024 (nur in Großbritannien zugänglich)
- Guidelines on Non-neurogenic Female LUTS; European Association of Urology (updated March 2022)
- Guidelines on Urinary Incontinence in Adults; European Association of Urology (2020)
Über den AutorVollständige Biografie anzeigen

Dr Rachel Hudson, MRCGP
Allgemeinmediziner und Medizinischer Autor
MBChB, MRCGP (2008), BSc (Medical Science), DFSRH, DRCOG, DCH
Dr. Rachel Hudson ist eine NHS-Ärztin, die im Nordwesten Englands arbeitet.
Über den RezensentenVollständige Biografie anzeigen

Dr Philippa Vincent, MRCGP
Allgemeinmediziner, Medizinischer Autor
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent ist ein NHS-Arzt, der in Nordlondon arbeitet.
Artikelverlauf
Die Informationen auf dieser Seite wurden von qualifizierten Klinikern verfasst und begutachtet.
Artikel auch verfügbar in Englisch, Deutsch, Spanisch, Französisch, Italienisch, Portugiesisch, Hindi, Hebräisch, Arabisch, und Schwedisch.
Next review due: 14 Nov 2028
16. Nov. 2023 | Neueste Version

Fragen, teilen, verbinden.
Durchsuchen Sie Diskussionen, stellen Sie Fragen und teilen Sie Erfahrungen zu Hunderten von Gesundheitsthemen.

Fühlen Sie sich unwohl?
Bewerten Sie Ihre Symptome online kostenlos
Abonnieren Sie den Patienten-Newsletter
Ihre wöchentliche Dosis klarer, vertrauenswürdiger Gesundheitsberatung - geschrieben, um Ihnen zu helfen, sich informiert, selbstbewusst und in Kontrolle zu fühlen.
Durch das Abonnieren akzeptieren Sie unsere Datenschutzrichtlinie. Sie können sich jederzeit abmelden. Wir verkaufen Ihre Daten niemals.
Mehr über Niere und Harnwege
- Akutes Nierenversagen
- Bettnässen
- Blasenkrebs
- Blut im Urin
- Diabetes insipidus
- Diabetische Nierenerkrankung
- Glomerulonephritis
- IgA-Nephropathie
- Intravenöse Urographie
- Ketone im Urin
- Symptome des unteren Harntrakts bei Männern
- Symptome des unteren Harntrakts bei Frauen
- Medikamente gegen Harndrang und Inkontinenz
- Urinprobe aus dem Mittelstrahl
- Überaktives Blasensyndrom
- Polyzystische Nierenerkrankung
- Proteinurie
- Dranginkontinenz
- Harnwegsinfektionen
- Harnwegsinfektion in der Schwangerschaft