Psoriasis-Arthritis
Begutachtet von Dr Hayley Willacy, FRCGP Zuletzt aktualisiert von Dr Colin Tidy, MRCGPZuletzt aktualisiert 9. Jan 2024
Erfüllt die Anforderungen des Patienten Richtlinien des Patienten
- HerunterladenHerunterladen
- Teilen
- Language
- Diskussion
- Audio-Version
In dieser Serie:PsoriasisGuttate PsoriasisNagelpsoriasis
Psoriatic arthritis causes inflammation, pain and swelling of joints in some people who have psoriasis. Other parts of the body may also be affected. For example, inflammation may also affect tendons and ligaments.
The severity can vary from mild to severe. In some cases, affected joints become damaged which can cause disability. Treatments include medication to ease pain, and medication to slow down the progression of the disease. Surgery is sometimes needed if a joint or tendon becomes badly damaged.
In diesem Artikel:
Videoauswahl für Arthritis
Lesen Sie unten weiter
Was ist Psoriasis-Arthritis?
Psoriatic arthritis is a particular type of arthritis that develops in some people who also have psoriasis. Arthritis means inflammation of the joints.
Psoriasis is a common skin condition which typically causes patches (plaques) of red, scaly skin to develop.
Who develops psoriatic arthritis?
Zurück zum InhaltAbout 1 person in 10 with psoriasis develops psoriatic arthritis. About 2 in 100 people develop psoriasis at some stage in their lives.
In most cases, the arthritis develops after the psoriasis - most commonly within 10 years after the psoriasis first develops. However, in some cases the arthritis develops much later.
In a small number of cases the arthritis develops first, sometimes months or even years before the psoriasis develops. Men and women are equally affected.
Psoriasis most commonly first occurs between the ages of 15 and 25 and psoriatic arthritis most commonly develops between the ages of 25 and 50. However, both psoriasis and psoriatic arthritis can occur at any age, including in childhood.
Hinweis: people with psoriasis also have the same chance as everyone else of developing other types of arthritis such as rheumatoide Arthritis und Osteoarthritis. Psoriatic arthritis is different, and is a particular type of arthritis that occurs only in some people with psoriasis.
Lesen Sie unten weiter
Symptoms of psoriatic arthritis
Zurück zum InhaltJoint symptoms
The common main symptoms are:
Pain and stiffness of affected joints.
Swelling and redness around the affected joints.
The stiffness is usually worse first thing in the morning, or after you have been resting.
The inflammation causes swelling and redness around the affected joints. Over time, in some cases, the inflammation can damage the joint. The extent of joint damage can vary from case to case.
On average, the joint damage tends not to be as bad or as disabling as occurs with rheumatoid arthritis. However, joint damage can cause significant deformity and disability in some cases.
Inflammation around tendons
This is quite common. It probably occurs because the tissue which covers tendons is similar to the synovium around the joints.
A common site is inflammation of the tendons of the fingers. Affected fingers may become swollen and 'sausage-shaped' if there is inflammation in the finger joints and overlying tendons at the same time.
The Achilles tendon is another common site, especially where the tendon attaches to the bone. Various other tendons around the body are sometimes affected.
The skin rash of psoriasis
See the separate leaflet called Psoriasis for more details.
Andere Symptome
Dazu gehören:
Inflammation of ligaments.
Pitting of the nails (tiny depressions in the nail), and separation of the nail from the nail bed. See the separate leaflet called Psoriatic Nail Disease for more details.
Inflammation in other parts of the body. Inflammation of the front of the eyes (conjunctivitis) and/or of the iris around the pupil (Uveitis) are the most common examples. Rarely, inflammation can develop in other places such as the aorta (a main blood vessel) or lungs.
What causes psoriatic arthritis?
Zurück zum InhaltThe exact cause is not known. Inflammation develops in the synovium of affected joints (the tissue that surrounds each joint) and sometimes in other parts of the body such as tendons and ligaments.
It is not clear what triggers the inflammation. It seems that the immune system is affected in some way, attacking healthy tissue, which leads to inflammation.
Genetic factors seem to be important, as psoriatic arthritis occurs more commonly in people who have a family history of psoriatic arthritis. However, it is not a straightforward hereditary condition.
It is thought that a virus or other factor in the environment may trigger the immune system to cause the inflammation in people who are genetically prone to it.
Lesen Sie unten weiter
Which joints are affected in psoriatic arthritis?
Zurück zum InhaltAny joint can be affected. However, there are five main patterns of this disease. Affected people tend to fall into one of these patterns, although many people overlap between two or more patterns. The patterns are:
Asymmetrical oligoarticular arthritis
This is a common pattern and tends to be the least severe. 'Oligo' means 'a few'. In this pattern usually fewer than five joints are affected at any time.
A common situation is for one large joint to be affected (for example, a knee) plus a few small joints in the fingers or toes.
Symmetrical polyarthritis
This pattern is also quite common. Symmetrical means that, if a joint is affected on the right side of the body (such as a right elbow), the same joint on the left side is also often affected.
Polyarthritis means that several joints become inflamed, usually including several of the smaller joints in the wrists and fingers.
Spondylitis with or without sacroiliitis
This pattern occurs in about 1 in 20 cases. 'Spondylitis' means inflammation of the joints and discs of the spine. 'Sacroiliitis' means inflammation of the joint between the lower spine (sacrum) and the pelvis. Back pain is the main symptom.
Distal interphalangeal joint predominant
This is a rare pattern where the small joints closest to the nails (distal interphalangeal joints) in the fingers and toes are mainly affected, causing swollen fingers and toes.
Arthritis mutilans
This is a rare pattern where a severe arthritis causes marked deformity to the fingers and toes.
How is psoriatic arthritis diagnosed?
Zurück zum InhaltThere is no test which clearly diagnoses early psoriatic arthritis. When you first develop symptoms of arthritis it can be difficult for a doctor definitely to confirm that you have psoriatic arthritis. This is because there are many other causes of arthritis.
However, if you have developed psoriasis within the previous few years and then an arthritis develops, there is a good chance that the diagnosis is psoriatic arthritis.
In time, the pattern and course of the disease tend to become typical and a doctor may then be able to give a firm diagnosis.
Some tests may be done, such as Bluttests und Röntgenaufnahmen. These can help to rule out other types of arthritis. For example, most people with rheumatoid arthritis have an antibody in their blood called rheumatoid factor. This does not usually occur in psoriatic arthritis.
Also, the X-ray appearance of joints affected by psoriatic arthritis tends to be different to that seen in rheumatoide Arthritis und Osteoarthritis.
How does psoriatic arthritis progress?
Zurück zum InhaltOnce the disease is triggered, psoriatic arthritis is usually a chronic relapsing condition. Chronic means that it is persistent. Relapsing means that, at times, the disease flares up (relapses) and, at other times, it settles down.
There is usually no apparent reason why the inflammation may flare up for a while and then settle down.
The amount of joint damage that may eventually develop can range from mild to severe. At the outset of the disease, it is difficult to predict for an individual how badly the disease will progress. However, modern medicines that are commonly used these days aim to suppress the inflammation in the joints and prevent joint damage.
Treatment for psoriatic arthritis
Zurück zum InhaltThe main aims of treatment are:
To reduce pain and stiffness in affected joints and tendons as much as possible.
To prevent joint damage and deformity as much as possible.
To minimise any disability caused by pain or joint damage.
Treatment aim 1 - to reduce pain and stiffness
Zurück zum InhaltDuring a flare-up of inflammation, if you rest the affected joint(s) it helps to ease pain. Special wrist splints, footwear, gentle massage, or applying heat may also help. Medication is also helpful. Medicines which may be advised by your doctor to ease pain and stiffness include the following:
Non-steroidal anti-inflammatory medicines
These are known as 'Nichtsteroidale entzündungshemmende Medikamente (NSAIDs)' and are sometimes just called 'anti-inflammatories'. They are good at easing pain and stiffness.
There are many types and brands. Each is slightly different to the others, and side-effects may vary between brands.
To decide on the right brand to use, a doctor has to balance how powerful the effect is against possible side-effects and other factors. Usually one can be found to suit. However, it is not unusual to try two or more brands before finding one that suits you best.
Hinweis: it is thought that some anti-inflammatories may make the rash of psoriasis worse in some people. Tell your doctor if you think that your psoriasis has become worse since starting an anti-inflammatory. An alternative anti-inflammatory or a different type of painkiller may be an option.
Schmerzmittel
Paracetamol often helps. This does not have any anti-inflammatory action but is useful for pain relief in addition to, or instead of, an anti-inflammatory. Codein is another painkiller that is sometimes used.
Steroide
Ein injection of steroid directly into a joint or inflamed tendon is sometimes used to treat a bad flare-up in one particular joint or tendon. Steroids are good at reducing inflammation.
Hinweis: anti-inflammatories, ordinary painkillers, and steroids ease the symptoms. However, they do not alter the progression of the disease or prevent joint damage. You do not need to take them if symptoms settle between flare-ups.
Treatment aim 2 - to prevent joint damage as much as possible
Zurück zum InhaltDisease-modifying medicines
There are a number of medicines called disease-modifying antirheumatic drugs (DMARDs).
DMARDs are commonly used as early as possible after a diagnosis of psoriatic arthritis is made. They aim to suppress inflammation and reduce the damaging effect of the disease on the joints.
They work by blocking the effects of chemicals involved in causing joint inflammation. Sulfasalazin und Methotrexat are the most commonly used DMARDs for psoriatic arthritis; however, there are others.
DMARDs have no immediate effect on pains or inflammation. It can take up to 4-6 months before you notice any effect. Therefore, it is important to keep taking a DMARD as prescribed, even if it does not seem to be working at first.
After starting a DMARD, many people continue to take an anti-inflammatory for several weeks until the DMARD starts to work. Once a DMARD is found to help, the dose of the anti-inflammatory can be reduced or even stopped. It is then usual to take a DMARD indefinitely.
Each DMARD has different possible side-effects. If one does not suit, a different one may be fine. Some people try two or three DMARDs before one is found to suit. (Some side-effects can be serious. These are rare and include damage to the liver and blood-producing cells. Therefore, it is usual to have regular tests - usually blood tests - whilst you take a DMARD. The tests look for some possible side-effects before they become serious.)
Some DMARDs also have a beneficial effect on reducing the rash of psoriasis.
Newer disease-modifying medicines
A new class of recently developed medicines modify the effect of TNF alpha. The chemical TNF alpha plays an important role in causing inflammation in joints and skin.
Blocking the effect of TNF alpha has been shown to reduce damage to joints and to reduce symptoms. Medicines which modify or block the effect of TNF alpha include etanercept, infliximab, adalimumab, certolizumab pegol, secukinumab and golimumab.
Other newer disease-modifying medicines used to treat psoriatic arthritis include apremilast, tofacitinib, ixekizumab, ustekinumab, guselkumab, upadacitinib, risankizumab and bimekizumab.
The National Institute for Health and Care Excellence (NICE) guidelines advise that etanercept, infliximab, adalimumab or golimumab should be offered as an option for treating adults with psoriatic arthritis when:
The person has arthritis with three or more tender joints and three or more swollen joints; und
When at least two other DMARDs, given on their own or together, haven't worked.
NICE recommends that other newer disease-modifying medicines as listed above can be used if a tumour necrosis factor (TNF) alpha inhibitor can't be used or hasn't been effective.
Treatment aim 3 - to minimise disability as much as possible
Zurück zum InhaltAs far as possible, try to keep active. The muscles around the joints will become weak if they are not used. Regular exercise may also help to reduce pain and improve joint function. Swimming is a good way to exercise many muscles without straining joints too much.
If such things as your grip or mobility become poor, an occupational therapist may advise on adaptations to the home to make daily tasks easier.
If severe damage occurs to a joint, joint replacement surgery may be an option.
Sometimes an operation is needed to fix a damaged tendon.
Andere Behandlungen
Zurück zum InhaltSome people try complementary therapies such as special diets, bracelets, acupuncture, etc, to help ease arthritis. There is little research evidence to say how effective such treatments are for psoriatic arthritis.
In particular, beware of paying a lot of money to people who make extravagant claims of success. For advice on the value of any treatment it is best to consult a doctor, or contact one of the groups below.
What is the outlook for people with psoriatic arthritis?
Zurück zum InhaltThe severity of psoriatic arthritis is variable and can be mild or severe. In about half of cases there is a progressive disease, eventually leading to loss of function in affected joints.
However, symptoms can often be well controlled with medication. Because of the newer medicines, in particular the newer disease-modifying medicines, the outlook (prognosis) for a person who is diagnosed with psoriatic arthritis now is likely to be much better than it used to be.
Understanding joints
Zurück zum InhaltNormal joint
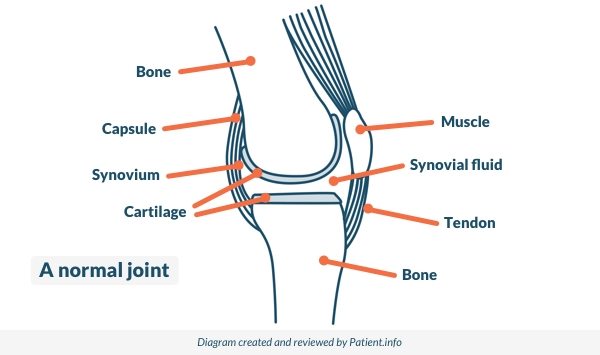
© Patient.info
The place where two bones meet is called a joint. Joints allow movement and flexibility of various parts of the body. The movement of the bones is caused by muscles which pull on tendons that are attached to bone.
Cartilage covers the end of bones. Between the cartilage of two bones which form a joint there is a small amount of thick fluid called synovial fluid. This fluid 'lubricates' the joint, which allows smooth movement between the bones.
The synovial fluid is made by the synovium. This is the tissue that surrounds the joint. The outer part of the synovium is called the capsule. This is tough, gives the joint stability, and stops the bones from moving 'out of joint'. Surrounding ligaments and muscles also help to give support and stability to joints.
Patientenempfehlungen für Arthritis

Knochen, Gelenke und Muskeln
Reaktive Arthritis
Reaktive Arthritis ist eine Art von Arthritis, bei der sich die Gelenke nach einer Infektion in einem anderen Teil des Körpers entzünden. Zum Beispiel kann nach einer schweren Durchfallerkrankung einige Wochen später ein schmerzendes Knie auftreten. Die Symptome dauern in der Regel zwischen einigen Wochen und einigen Monaten an. Entzündungshemmende Medikamente lindern normalerweise die Schmerzen. Manchmal sind weitere Behandlungen erforderlich. Dies ist eine ungewöhnliche Erkrankung, die in der Regel von einem Spezialisten behandelt wird.
von Dr. Rosalyn Adleman, MRCGP

Knochen, Gelenke und Muskeln
Arthritis
Arthritis bedeutet Entzündung in einem Gelenk (wie Ihrem Knie, Ihrer Hüfte, Ihrem Ellbogen oder Ihren Fingern). Es ist ein häufiges Problem und betrifft im Allgemeinen ältere Menschen, obwohl es einige seltene Erkrankungen gibt, die bei Kindern und Jugendlichen Arthritis verursachen. Es gibt viele Arten von Arthritis. Einige verursachen kurzfristige Schmerzen in den Gelenken und lösen sich dann vollständig auf, andere können langfristige Probleme verursachen und dauerhaft beeinflussen, wie sich Ihre Gelenke bewegen. Dieses Merkblatt erklärt ein wenig darüber, wie Gelenke funktionieren, und geht dann in leicht verständlicher Sprache auf die Hauptursachen von Arthritis ein.
von Dr. Toni Hazell, MRCGP
Weiterführende Lektüre und Referenzen
- Etanercept, Infliximab und Adalimumab zur Behandlung der Psoriasis-Arthritis; NICE-Technologiebewertungsleitlinie, August 2010
- Golimumab zur Behandlung von Psoriasis-Arthritis; NICE-Technologiebewertungsleitlinie, April 2011
- Psoriasis: Die Beurteilung und Behandlung von Psoriasis; NICE Klinische Leitlinie (Oktober 2012 - zuletzt aktualisiert September 2017)
- Ustekinumab zur Behandlung von aktiver Psoriasis-Arthritis (schnelle Überprüfung der Technologie-Bewertungsempfehlung 313); NICE-Technologiebewertungsleitlinie, Juni 2015 - zuletzt aktualisiert im März 2017
- Guselkumab zur Behandlung von aktiver Psoriasis-Arthritis nach unzureichender Reaktion auf DMARDs; NICE Technology Appraisal Guidance, June 2021
- Upadacitinib zur Behandlung von aktiver Psoriasis-Arthritis nach unzureichender Reaktion auf DMARDs; NICE Technologie-Bewertungsleitlinie, Februar 2022
- Risankizumab zur Behandlung von aktiver Psoriasis-Arthritis nach unzureichender Reaktion auf DMARDs; NICE Technologie-Bewertungsleitlinie, Juli 2022
- Guselkumab zur Behandlung von aktiver Psoriasis-Arthritis nach unzureichender Reaktion auf DMARDs; NICE Technologie-Bewertungsleitlinie, August 2022
- Bimekizumab zur Behandlung von aktiver Psoriasis-Arthritis; Technologie-Bewertungsrichtlinien, Oktober 2023
- Psoriasis; NICE CKS, September 2023 (nur für UK-Zugang)
Lesen Sie unten weiter
Artikelverlauf
Die Informationen auf dieser Seite wurden von qualifizierten Klinikern verfasst und begutachtet.
Nächste Überprüfung fällig: 7. Jan 2029
9. Jan. 2024 | Neueste Version

Fragen, teilen, verbinden.
Durchsuchen Sie Diskussionen, stellen Sie Fragen und teilen Sie Erfahrungen zu Hunderten von Gesundheitsthemen.

Fühlen Sie sich unwohl?
Bewerten Sie Ihre Symptome online kostenlos
Abonnieren Sie den Patienten-Newsletter
Ihre wöchentliche Dosis klarer, vertrauenswürdiger Gesundheitsberatung - geschrieben, um Ihnen zu helfen, sich informiert, selbstbewusst und in Kontrolle zu fühlen.
Mit dem Abonnieren akzeptieren Sie unsere Datenschutzrichtlinie. Sie können sich jederzeit abmelden. Wir verkaufen Ihre Daten niemals.