Angina
Begutachtet von Dr Toni Hazell, MRCGPZuletzt aktualisiert von Dr Hayley Willacy, FRCGP Zuletzt aktualisiert 30. Jan 2023
Erfüllt die Anforderungen des Patienten Richtlinien des Patienten
- HerunterladenHerunterladen
- Teilen
- Language
- Diskussion
- Audio-Version
- Zu bevorzugten Quellen bei Google hinzufügen
In dieser Serie:Mikrovaskuläre AnginaKoronararterienspasmus
Angina is a pain that comes from the heart. It is usually caused by narrowing of the heart's blood vessels - the (coronary) arteries. Usual treatment includes a Statin medicine to lower your cholesterol level, low-dose aspirin to help prevent a heart attack, and a Betablocker medicine to help protect the heart and to prevent angina pains. An angiotensin-converting enzyme (ACE) inhibitor medicine is advised in some cases. Sometimes angioplasty or surgery are options to widen, or to bypass, narrowed arteries.
Auf einen Blick
Angina is chest pain that comes from the heart.
It usually occurs when your heart needs more blood than narrowed arteries can supply.
Symptoms include tightness across the chest, which may spread to your arms, jaw, or stomach.
The pain typically worsens with exertion and eases with rest, usually within 10 minutes.
If pain lasts longer than 10 minutes, or is more severe, call an ambulance immediately.
What is angina?
What is angina?
Angina is a pain that comes from the heart. Each year about 20,000 people in the UK develop angina for the first time. It is more common in people over the age of 50 years. It is also more common in men than in women. Sometimes it occurs in younger people.
This leaflet is about the common type of angina which is caused by narrowing in the coronary arteries of the heart. Sometimes angina can be caused by uncommon disorders of the heart valves or heart muscle.
What causes angina?
Heart with atheroma
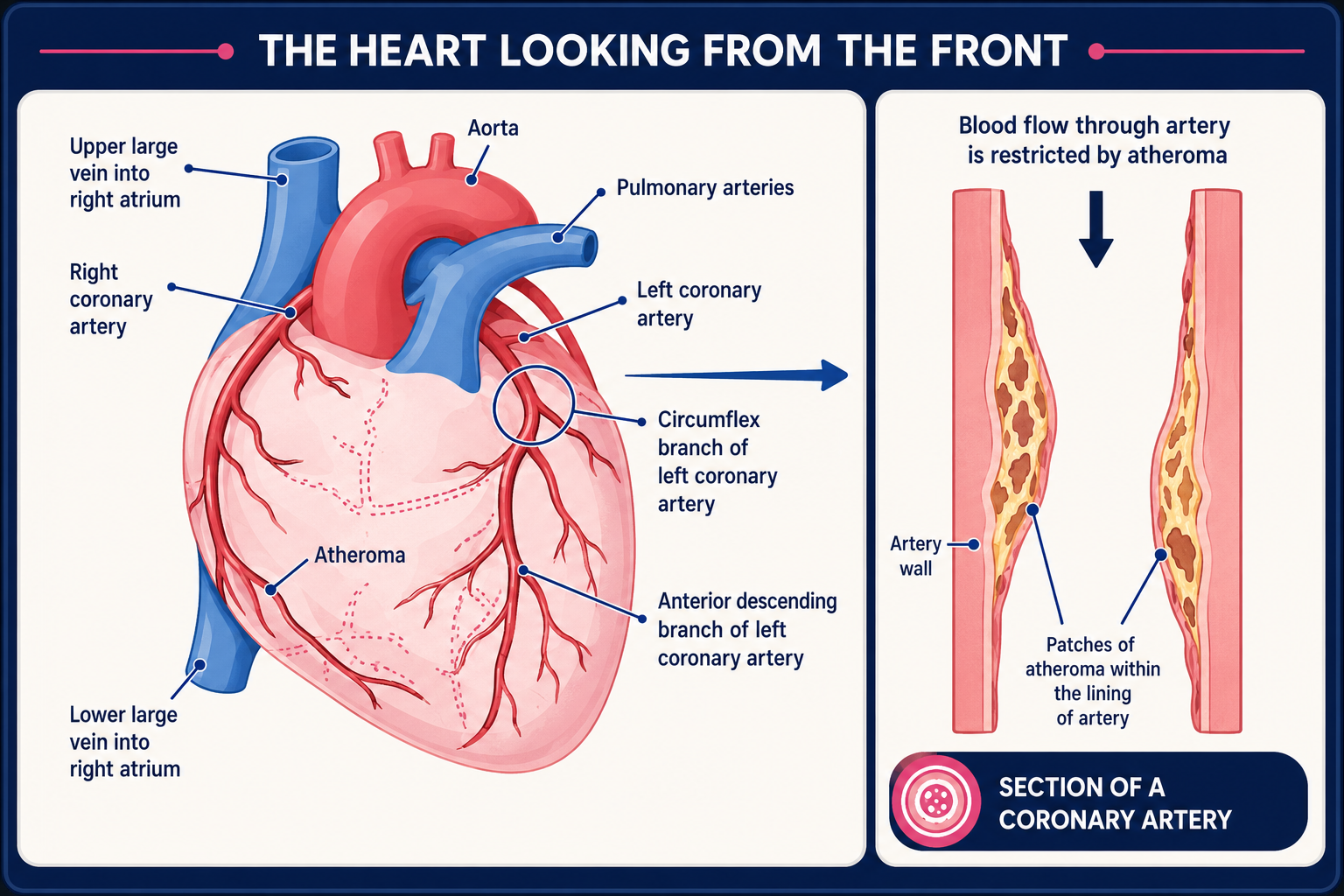
If you have angina, one or more of your heart (coronary) arteries are usually narrowed. This causes a reduced blood supply to a part, or parts, of your heart muscle.
The blood supply may be good enough when you are resting. When your heart works harder (when you walk fast or climb stairs and your heart rate increases) your heart muscle needs more blood and oxygen. If the extra blood that your heart needs cannot get past the narrowed coronary arteries, the heart responds with pain.
The narrowing of the arteries is caused by atheroma. See the separate leaflet called High Cholesterol for more information about atheroma.
Angina can also be caused by:
Spasm of the coronary arteries. Read more about Koronararterienkrampf.
Other problems with the blood supply to the heart. Read more about cardiac syndrome X (microvascular angina).
Angina symptoms
Typical and common angina symptoms
Pain, ache, discomfort or tightness that you feel across the front of the chest.
The pain is usually worse when you exert yourself. For example, when you walk up a hill or against a strong, cold wind.
You may also, or just, feel the pain in your arms, jaw, neck or stomach.
An angina pain does not usually last long. It will usually ease within 10 minutes when you rest.
If you take some Glyceroltrinitrat (GTN) it should go within 1-2 minutes (see 'Glyceryl trinitrate' section, below).
Angina pain may also be triggered by other causes of a faster heart rate - for example, when you have a vivid dream or an argument. The pains also tend to develop more easily after meals.
See also the separate leaflet called Chest Pain.
Less typical symptoms that sometimes occur
Some people have non-typical pains - for example, pains that develop when bending or eating.
If the symptoms are not typical then it is sometimes difficult to tell the difference between angina and other causes of chest pain, such as a pulled muscle in the chest or heartburn.
Some people with angina also become breathless when they exert themselves. Occasionally, this is the only symptom and there is no pain.
What tests will I have for angina?
If you have suspected angina, tests are usually advised:
Bluttests to check for anaemia, thyroid problems, kidney problems, a high blood sugar (glucose) level and a high cholesterol level, as these may be linked with angina.
Ein Herzdiagramm (Elektrokardiogramm oder EKG). This can be useful. However, a routine ECG may be normal if you have angina. In fact, more than half of people with angina have a normal resting ECG.
How do doctors know that I have angina?
In many cases doctors can make the diagnosis based on the typical symptoms. No further tests may then be necessary. Tests are advised in some cases when the diagnosis is not clear, or sometimes to assess the severity of the condition. The tests that you have will depend on what is available locally and whether the test is suitable for you. One or more of these may be advised:
An ultrasound scan of the heart (echocardiogram, or 'echo').
A magnetic resonance imaging (MRI) scan can also show how your heart works under stress.
Belastungstest has been used for many years to diagnose and assess the severity of angina. However, this test is done less often these days due to more the more modern tests (listed above) becoming available. Current UK guidelines do not recommend using exercise testing to make the initial diagnosis of angina.
What can I do to help with angina?
Certain risk factors increase the risk of more fatty patches or plaques (atheroma) forming, which can make angina worse. Siehe den separaten Beipackzettel mit dem Titel Herz-Kreislauf-Erkrankungen (Atherom) für weitere Details.
Briefly, risk factors that can be modified and may help to prevent angina from becoming worse include:
Rauchen. If you smoke, you should make every effort to stop.
Hoher Blutdruck. Your blood pressure should be checked regularly, at least once a year, if you have angina. If it is high, it can be treated.
Wenn Sie übergewichtig sind, losing some weight is advised. Losing weight will reduce the amount of workload on your heart and also help to lower your blood pressure.
hohen Cholesterinspiegel. This should be treated if it is high.
Inaktivität. You should aim to do some moderate physical activity on most days of the week for at least 30 minutes. For example, brisk walking, swimming, cycling, dancing, gardening, etc. (Occasionally, angina is due to a heart valve problem where physical activity may not be so good. Ask your doctor to confirm that you can undertake regular physical activity.)
Ernährung. You should aim to eat a healthy diet. A healthy diet means:
At least five portions (and ideally 7-9 portions) of a variety of fruit and vegetables per day.
You should not eat much fatty food such as fatty meats, cheeses, full-cream milk, fried food, butter, etc. Ideally you should use low-fat, mono-unsaturated or polyunsaturated spreads.
Try to include 2-3 portions of fish per week, at least one of which should be oily (such as herring, mackerel, sardines, kippers, salmon, or fresh tuna).
If you eat red meat, it is best to eat lean red meat, or eat poultry such as chicken.
If you do fry, choose a vegetable oil such as sunflower, rapeseed or olive.
Try not to add salt to food. Limit foods which are salty.
Alcohol definitely has a harmful effect on heart health when consumed above the recommended guideline amounts - ie 14 units per week maximum with at least two completely alcohol-free days in the week. However when alcohol is consumed at a lower level than that, the effect on risks is less clear.
Angina treatment
The main aims of treatment are:
To prevent angina pains as much as possible and to ease pain quickly if it occurs.
To limit further deposits of fatty patches or plaques (atheroma) as much as possible. This prevents or delays the condition from worsening.
To reduce the risk of having a heart attack (myocardial infarction).
Treatments that are advised in most cases
In addition to the lifestyle factors listed above, the treatments for angina include:
Glyceryl trinitrate (GTN) to relieve an angina episode.
Aspirin or another antiplatelet medicineto reduce the risk of blood clots.
A beta-blocker medicine to prevent the heart beating too fast.
Other treatments that may be advised
Other medicines to prevent angina pains
A beta-blocker may be sufficient to prevent angina pains but other medicines are available if required. They fall into three main groups:
Calciumkanalblocker (for example, Amlodipin).
Nitrate medicines (for example, isosorbide mononitrate).
Potassium-channel activators (for example, nicorandil).
Non-medicine treatments
Koronarangioplastie oder coronary artery bypass graft (CABG) surgery may be offered if:
You have pains not controlled by medicines; oder
The site and severity of the atheroma deposits are particularly suited to one of these treatments. In some cases this may even be if you have few or no pains, as the overall outlook may be improved in certain circumstances.
Common worries about angina
Straining the heart by exertion
This is a common worry. On the contrary, more physical activity is usually advised. You will normally be encouraged to exercise regularly. Physical activity helps to make the heart fitter and improves the blood supply to the heart muscle.
Geschlecht
Some people with angina worry that the physical effort of having sex will damage the heart. This is wrong and you do not need to stop having sex. If sex does bring on an angina pain, it may be helpful to take some GTN beforehand.
Driving and flying
There is usually no restriction for driving your own car unless pains occur at rest, with emotion or while driving. But, you must inform your insurance company if you have angina. People with PCV or LGV licences, who have angina, must stop driving and, in the UK, contact the DVLA.
As regards flying, in general, if you can climb 12 stairs and walk 100 metres on the level without pain or becoming very breathless, you are fit to fly as a passenger. People with frequent angina pains or unstable angina should avoid flying. Please note that your GP is not able to sign a form stating that you are fit to fly. This must be assessed by a doctor who has been specifically trained for this task.
Other points about angina
Stable angina and unstable angina
In most cases, angina pains come on with a certain amount of exertion and you can predict the level of exertion that triggers a pain. This situation is called stable angina. More than a million people in the UK have stable angina. It is common to have stable angina for many years and, with treatment, most pains can be prevented. Over months or years the pains may come on with a lesser amount of exertion if the condition gradually becomes worse.
If the pattern of your pain changes fairly suddenly and the pains develop after minimal exertion, or while you are resting, this is called unstable angina. This is an emergency and needs immediate medical care.
Prolonged pain
If you have a pain that lasts longer than 10 minutes, does not respond to your GTN or is different or more severe than usual, call an ambulance immediately. It may be unstable angina or a Herzinfarkt and immediate medical care is needed.
Impfung
People with angina should have the Pneumokokkenimpfung und der annual flu immunisation.
Patientenauswahl für Herzkrankheit
Herzgesundheit und Blutgefäße
Aortenstenose
Die Aortenklappe ist eine Herzklappe, die zwischen dem linken Ventrikel und der Aorta liegt. Bei der Aortenstenose öffnet sich die Aortenklappe, um Blut durchzupumpen, nicht so weit wie normalerweise. Die Öffnung zwischen dem linken Ventrikel und der Aorta ist daher verengt (stenosiert). Die Menge an Blut, die vom linken Ventrikel zur Aorta gelangen kann, ist daher reduziert. Je stärker die Klappe verengt ist, desto geringer ist die Menge an Blut, die durchkommen kann, und desto signifikanter sind die Symptome. In einigen Fällen tritt die Aortenstenose gleichzeitig mit der Aorteninsuffizienz auf.
von Dr. Philippa Vincent, MRCGP

Herzgesundheit und Blutgefäße
Bewertung des kardiovaskulären Gesundheitsrisikos
Eine Bewertung des kardiovaskulären Gesundheitsrisikos bietet eine genaue Schätzung Ihres Risikos, in den nächsten 10 Jahren eine Herz-Kreislauf-Erkrankung (z. B. Angina, Herzinfarkt, Schlaganfall oder periphere arterielle Erkrankung) zu entwickeln, und bietet Ihnen die Möglichkeit, Änderungen vorzunehmen, die dieses Risiko verringern. Wenn Sie bereits an einer Herz-Kreislauf-Erkrankung oder Diabetes leiden, muss Ihr Risiko nicht bewertet werden, da Sie bereits zur Hochrisikogruppe gehören.
von Dr. Colin Tidy, MRCGP
Häufig gestellte Fragen
Can angina last for days?
No, a typical angina pain does not usually last long. It will generally ease within 10 minutes when you rest. If the pain lasts longer than 10 minutes, does not respond to your GTN medication, or feels different or more severe than usual, you should call an ambulance immediately.
How long can you live with blocked arteries?
Many people live with narrowed coronary arteries for many years, especially with appropriate treatment and lifestyle changes. The aim of treatment for angina is to prevent the condition from worsening, reduce the risk of a heart attack, and manage pains effectively.
Why do angina pains tend to develop more easily after meals?
Angina pains can be triggered more easily after meals because digestion temporarily increases the workload on your heart as it pumps more blood to the digestive system. If your heart arteries are narrowed, this extra demand can lead to pain.
What is the difference between stable and unstable angina?
Stable angina refers to pains that occur predictably with a certain amount of exertion. With stable angina, you can usually anticipate what activities might trigger the pain. Unstable angina, however, is an emergency where the pattern of pain changes suddenly, developing with minimal exertion or even at rest. This requires immediate medical attention.
Do I need to stop driving if I have angina?
Generally, you usually do not have to restrict driving your own car unless you experience pains at rest, with emotion, or while actually driving. However, you must inform your insurance company if you have angina. For people with PCV or LGV licences, if you have angina, you must stop driving and contact the DVLA.
Weiterführende Literatur und Referenzen
- Beurteilung der Fahrtauglichkeit: Leitfaden für medizinische Fachkräfte; Fahrer- und Fahrzeugzulassungsbehörde
- Behandlung der stabilen Angina pectoris; Schottisches Netzwerk für interkollegiale Richtlinien - SIGN (April 2018)
- Saraste A, Knuuti J; ESC 2019 guidelines for the diagnosis and management of chronic coronary syndromes : Recommendations for cardiovascular imaging. Herz. 2020 Aug;45(5):409-420. doi: 10.1007/s00059-020-04935-x.
- Angina; NICE CKS, Oktober 2022 (nur für UK-Zugang)
- Mahtani AU, Padda IS, Johal GS; Cardiac Syndrome X.
- Hoek AG, van Oort S, Mukamal KJ, et al; Alcohol Consumption and Cardiovascular Disease Risk: Placing New Data in Context. Curr Atheroscler Rep. 2022 Jan;24(1):51-59. doi: 10.1007/s11883-022-00992-1. Epub 2022 Feb 7.
Über den AutorVollständige Biografie anzeigen

Dr Hayley Willacy, FRCGP
Allgemeinmediziner, Medizinischer Autor
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr. Hayley Willacy war eine NHS-Hausärztin, die in Nordwestengland arbeitete und 2022 nach 30 Jahren aus der klinischen Praxis ausschied.
Über den RezensentenVollständige Biografie anzeigen

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell hat ihren Abschluss an der St. Mary’s Hospital Medical School gemacht und ihr VTS am Northwick Park Hospital absolviert.
Artikelverlauf
Die Informationen auf dieser Seite wurden von qualifizierten Klinikern verfasst und begutachtet.
Artikel auch verfügbar in Englisch, Deutsch, Spanisch, Französisch, Italienisch, Portugiesisch, Hindi, Hebräisch, Arabisch, und Schwedisch.
Nächste Überprüfung fällig: 29. Jan 2028
30. Jan 2023 | Neueste Version

Fragen, teilen, verbinden.
Durchsuchen Sie Diskussionen, stellen Sie Fragen und teilen Sie Erfahrungen zu Hunderten von Gesundheitsthemen.

Fühlen Sie sich unwohl?
Bewerten Sie Ihre Symptome online kostenlos
Abonnieren Sie den Patienten-Newsletter
Ihre wöchentliche Dosis klarer, vertrauenswürdiger Gesundheitsberatung - geschrieben, um Ihnen zu helfen, sich informiert, selbstbewusst und in Kontrolle zu fühlen.
Durch das Abonnieren akzeptieren Sie unsere Datenschutzrichtlinie. Sie können sich jederzeit abmelden. Wir verkaufen Ihre Daten niemals.